(sigh) Once again, the Kansas Insurance Dept. is supremely unhelpful when it comes to providing information about individual & small group market health insurance premium rate changes. Not only are the ACA plans not listed in the state's SERFF database or on the department's website, even the actuarial memos available at the federal Rate Review website are heavily redacted.
As a result, I only have the actual enrollment numbers for a handful of carriers, preventing me from being able to calculate a properly weighted average. With enrollment data for three of the six carriers on the individual market, and based on an estimated total individual market enrollment of 110,000 Kansans, the average increase should be around 8.3%, give or take (the unweighted average is 9.8%).
For the small group market, I don't have any hard enrollment data, so can only run the unweighted average increase, which is around 7.2%.
As I noted last night, thanks to the federal Rate Review website finally being updated to include the final, approved 2022 rates for both the individual and small group markets in all 50 states (+DC), I've been able to fill in the missing data for my annual ACA Rate Change Project.
As I note there, the overall weighted average looks like it'll be roughly +3.5% nationally.
Normally I write up a separate entry for both the preliminary and approved rate changes in each individual state, but it seems like overkill to create 14 separate entries at once. Besides, in many of these states there's been few if any changes between the preliminary and approved rate changes.
(sigh) Once again, the Kansas Insurance Dept. is supremely unhelpful when it comes to providing information about individual & small group market health insurance premium rate changes. Not only are the ACA plans not listed in the state's SERFF database or on the department's website, even the actuarial memos available at the federal Rate Review website are heavily redacted. As a result, I only have the actual enrollment numbers for a handful of carriers, preventing me from being able to calculate a weighted average (or to estimate the state's total ACA enrollment size, for that matter).
The unweighted average rate increase on Kansas' individual market is +8.3%, and it's +5.6% for the small group market, anyway.
I've once again relaunched my project from last fall to track Medicaid enrollment (both standard and expansion alike) on a monthly basis for every state dating back to the ACA being signed into law.
Kansas is one of 12 states which still hasn't expanded Medicaid eligibility under the ACA (13 if you include Missouri, whose voters expanded the program last year...but which the state legislature refuses to fund).
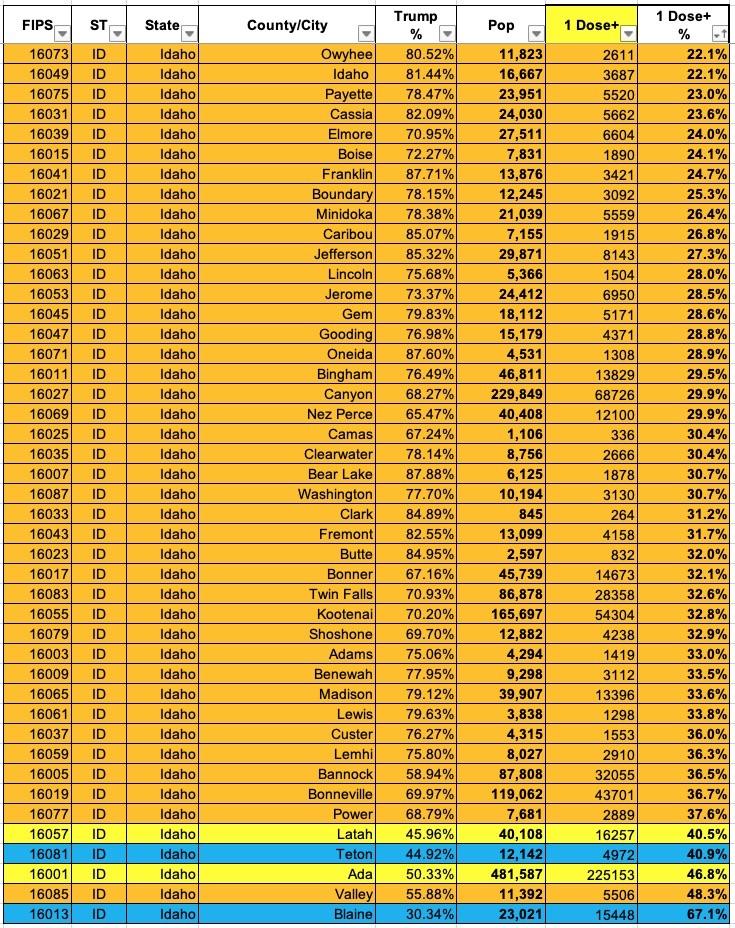
Now that I've developed a standardized format/layout & methodology for tracking both state- and county-level COVID vaccination levels by partisan lean (which can also be easily applied to other variables like education level, median income, population density, ethnicity, etc), I've started moving beyond my home state of Michigan.
NOTE: This is an updated version of a post from a couple of months ago. Since then, there's been a MASSIVELY important development: The passage of the American Rescue Plan, which includes a dramatic upgrade in ACA subsidies for not only the millions of people already receiving them, but for millions more who didn't previously qualify for financial assistance.
Much has been written by myself and others (especially the Kaiser Family Foundation) about the fact that millions of uninsured Americans are eligible for ZERO PREMIUM Bronze ACA healthcare policies.
I say "Zero Premium" instead of "Free" because there's still deductibles and co-pays involved, although all ACA plans also include a long list of free preventative services from physicals and blood screenings to mammograms and immunizations with no deductible or co-pay involved.
Once again, I'm afraid the actuarial memos for Kansas' 2021 individual and small group market carriers are either absent or redacted, so I have to run unweighted average rate changes, which are likely off significantly (for instance, the individual market is +7.8% unweighted, but if it turns out that, say, Oscar Insurance has 95% of the market share, the weighted average would be more like a 7% decrease).
Unfortuantely, without knowing the actual enrollment data for each carrier, this is the best I can do for now. The small group market's unweighted average increase is 8.2%.
TOPEKA, Kan. (KWCH) Gov. Laura Kelly and Republican leadership announce an agreement on Medicaid expansion in Kansas.
During a press conference on Thursday, the governor said the program would be funded by the hospital administrative fee. At this time, it's unknown if that fee would be passed on to patients.
Kelly said the hospitals have endorsed the program.
Kansas Senate GOP Majority Leader Jim Denning said the bill would be pre-filed on Thursday with 22 co-sponsors.
If passed in the Kansas Senate and House, the full expansion would go into effect no later than Jan. 1.
(Obviously that's January 1st of 2021 at this point, of course)
Here's some live tweeting of the event by a Kansas-based political reporter:
I didn't have the actual enrollment data for the individual carriers when I ran the numbers for Kansas in August, so I had to go with an unweighted average unsubsidized 2020 premium rate change. At the time, that came in at a 3.1% reduction.
Since then, I've dug up the hard enrollment numbers, and just this morning CMS finally posted the final, approved 2020 rate changes. The weighted average comes in at a slight increase o 0.3% statewide:
Cigna extended its individual healthcare exchange products for the 2020 plan year, the insurer said Sept. 18.
For 2020, individuals can purchase individual health plans in 19 markets across 10 states. The expansions will take place in counties in Kansas, South Florida, Utah, Tennessee and Virginia. The other states include Arizona, Colorado, Illinois and North Carolina.
The plans will be available for purchase on the individual marketplace during the 2020 open enrollment period, which begins Nov. 1. Plans will take effect Jan. 1.





{kind=link}