Now that I've developed a standardized format/layout & methodology for tracking both state- and county-level COVID vaccination levels by partisan lean (which can also be easily applied to other variables like education level, median income, population density, ethnicity, etc), I've started moving beyond my home state of Michigan.
As I noted recently, I've relaunched my project from last fall to track Medicaid enrollment (both standard and expansion alike) on a monthly basis for every state dating back to the ACA being signed into law.
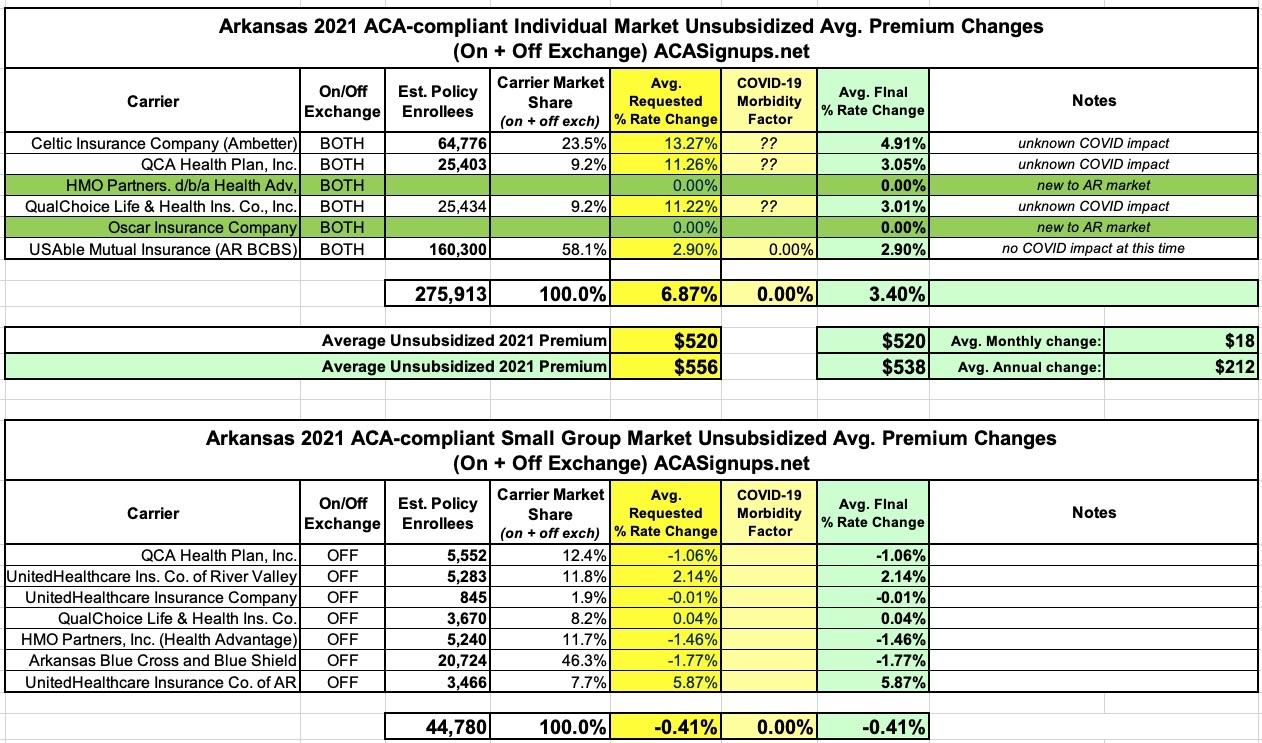
In early August, the Arkansas Insurance Dept. posted the preliminary 2021 rate filings for the individual & small group market. At the time, the carriers were requesting average increases of 7.0% for ACA indy market plans and a slight drop of 0.3% for the small group market.
The approved rate filings have now been published, and the increases have been cut in half on the individual market to just 3.4%, while the small group market is slightly lower still (-0.4%) due to a revision in the estimated number of current enrollees:
Insurance companies offering individual and small group health insurance plans are required to file proposed rates with the Arkansas Insurance Department for review and approval before plans can be sold to consumers.
The Department reviews rates to ensure that the plans are priced appropriately. Under Arkansas Law (Ark. Code Ann. § 23-79-110), the Commissioner shall disapprove a rate filing if he/she finds that the rate is not actuarially sound, is excessive, is inadequate, or is unfairly discriminatory.
The Department relies on outside actuarial analysis by a member of the American Academy of Actuaries to help determine whether a rate filing is sound.
Below, you can review information on the proposed rate filings for Plan Year 2020 individual and small group products that comply with the reforms of the Affordable Care Act.
Users will only be able to view the public details of the filing, as certain portions are deemed confidential by law (Ark. Code Ann. § 23-61-103).
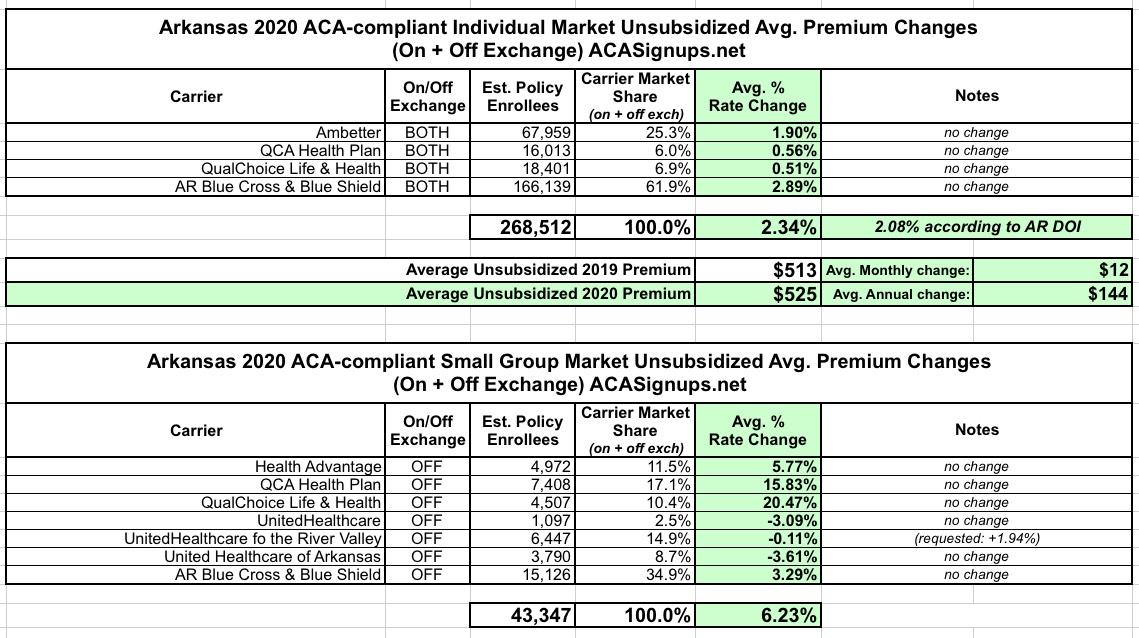
The Arkansas Insurance Dept. just posted their approved 2020 individual and small group market premium rate change requests. For the most part it's pretty straightforward: Individual market premiums are increasing about 2.3% statewide, while small group plans are going up 6.2% overall. This is virtually unchanged from their preliminary rate requests in July, although a single small group carrier had their request reduced from +2% to -0.1%, lowering the overall weighted average by a mere 0.2 points:
But that's not all! In addition to the actual 2018 MLR rebates, I've gone one step further and have taken an early crack at trying to figure out what 2019 MLR rebates might end up looking like next year (for the Individual Market only). In order to do this, I had to make several very large assumptions:
The Arkansas Insurance Dept. just posted their preliminary 2020 individual and small group market premium rate change requests. For the most part it's pretty straightforward: Individual market premiums are increasing about 2.3% statewide, while small group plans are going up 6.5% overall.
However, there's two interesting things to note about Arkansas' individual market: First, unlike most states where over 70% of enrollees do so through the ACA exchange, in Arkansas it's more like 20%, with nearly 80% are enrolled off-exchange. The main reason for this is the state's unique "Private Option" Medicaid expansion waiver, in which around 252,000 residents who would otherwise be enrolled in Medicaid itself are instead enrolled in enhanced ACA individual market policies...with the state paying for their premiums.
And since I was too swamped with other stuff, I didn't have a chance to write about it until now. A bunch of other outlets have already posted the details, so here's Dylan Scott of Vox.com to save me the trouble:
A federal district judge has blocked Medicaid work requirements approved by the Trump administration in Arkansas and Kentucky.
Last week, the state of Arkansas released its latest round of data on implementation of its Medicaid work reporting requirement – the first in the country to be implemented. As readers of SayAhhh! know, over 18,000 lost coverage in 2018 as a result of not complying with the new reporting rules. And the policy is clearly failing to achieve its purported goal – incentivizing work – with less than 1% of those subject to the new policy newly reporting work or community engagement activities.