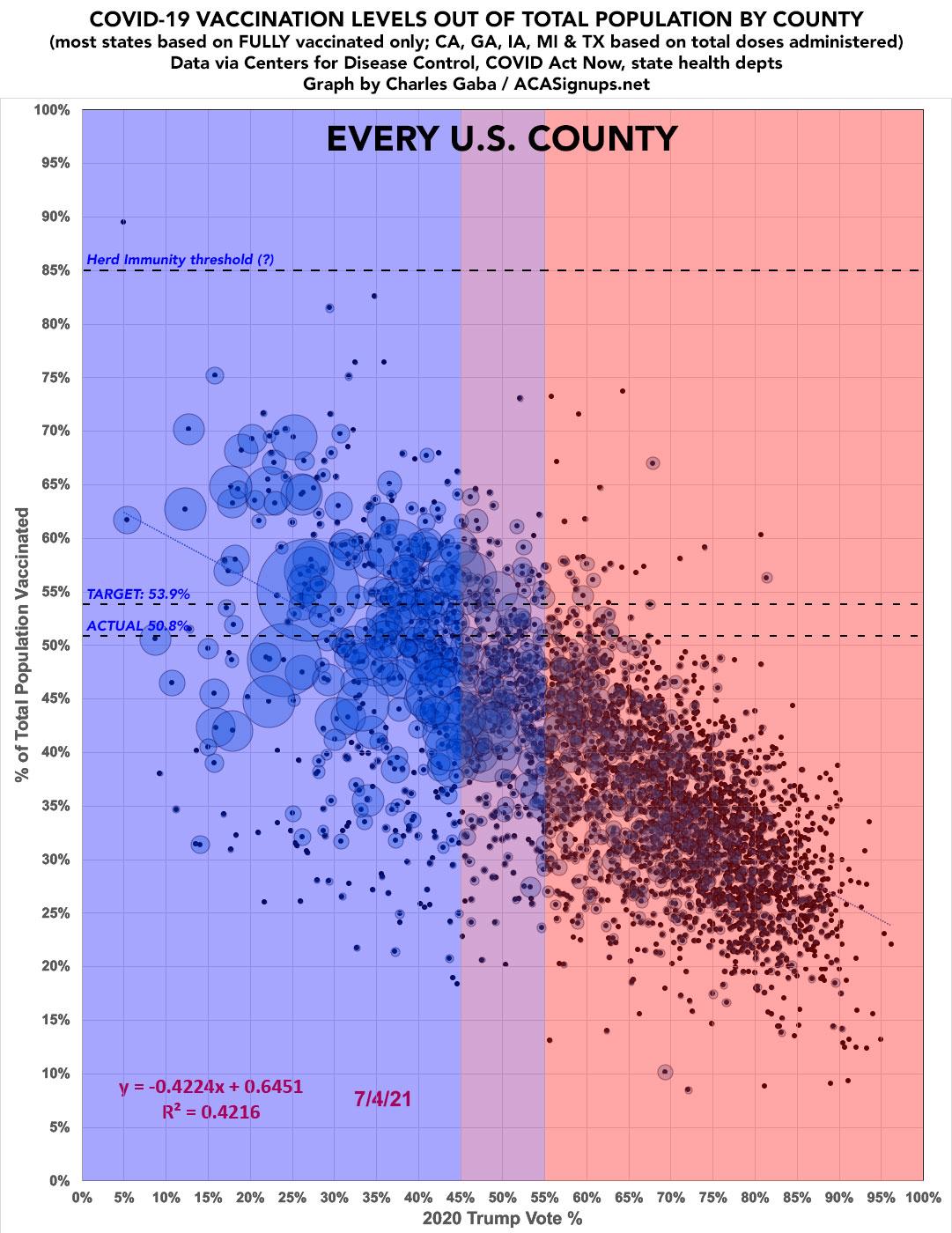
As I've been noting for months (and as the mainstream press has finally started picking up on), while there are several factors explaining why so many people haven't gotten vaccinated yet, the single biggest determining factor is their political lean and, even more specifically, who they voted for President last fall.
However, there are some outliers, as you would expect when you're looking at a nation of over 330 million people.
According to the latest data, if you take the original "every county" graph...
It's been over a month since I last ran a scatter plot displaying current COVID-19 vaccination rates across every COUNTY nationwide according to the 2020 election results...all 3,100+ of them. With today being the 4th of July, which also happens to be the target date for President Biden's call for at least 70% of all U.S. adults to have received their first vaccination shot.
Oklahoma's Medicaid Expansion will Provide Access to Coverage for 190,000 Oklahomans
Nearly 120,000 People Will Begin Receiving Full Medicaid Benefits on July 1
The Centers for Medicare & Medicaid Services (CMS) announced today that approximately 190,000 individuals between the ages of 19-64 in Oklahoma are now eligible for health coverage, thanks to Medicaid expansion made possible by the Affordable Care Act (ACA). On June 1, 2021, the state began accepting applications, and to date, over 120,000 people have applied for and were determined eligible to receive coverage. On July 1, these individuals will receive full Medicaid benefits, including access to primary and preventive care, emergency, substance abuse, and prescription drug benefits. Thanks to the American Rescue Plan (ARP), Oklahoma is eligible to receive additional federal funding for their Medicaid program, estimated to be nearly $500 million over two years. It is estimated that an additional 70,000 people in Oklahoma who have not yet applied are now eligible for coverage under Medicaid.
With the pace of Americans getting vaccinated slowing down to the point that we're not gonna quite meet President Biden's 4th of July target nationally (70% of adults receiving their first COVID-19 vaccination shot), there's a whole lot of hand-wringing about how much of the problem is access (i.e., people not being able to get time off of work, not having transportation to the clinic to get the shot, etc), how much of it is hesitancy (concerns about safety/efficacy, etc), and how much of it is about...well, to put it gently, being a lost or damaged soul.
Well, a new poll conducted by YouGov for Yahoo News may help answer that question (h/t Richard Skinner for the heads up). The poll, of nearly 1,600 U.S. adults, was conducted from June 22 - 24th. I've reformatted the relevant question below to fit better on this site.
The actual question as worded was: "How would you describe your personal situation regarding COVID-19 vaccines?"
Two weeks left to apply for private health insurance during special enrollment period
New cost savings available when you apply through MNsure
ST. PAUL, Minn.—Do you lack health insurance or are you currently enrolled in a health plan outside of MNsure? Don’t wait to act—you have until Friday, July 16, 2021 to apply and enroll in a plan this summer thanks to MNsure’s special enrollment period, designed to help more Minnesotans get the security of health insurance during the COVID-19 pandemic.
The COVID-19 Special Enrollment Period runs through August 15th in most states, but in Minnesota it's only available through July 15th.
To explore your options, visit MNsure.org and select “COVID special enrollment” on the homepage.
Health insurance is more affordable than ever for thousands of Minnesotans who enroll in private health plans through MNsure, thanks to the American Rescue Plan.
It's been clear for a couple of weeks now that, while many individual states have already long since surpassed it, nationally we aren't going to quite achieve President Biden's goal of at least 70% of U.S. adults getting their first COVID-19 vaccination shot.
That's around 9 million adults shy of the 7/04 target...with only around 300K - 400K adults getting their first shot each day. We're likely to end up around 7.7 million short, or right around 67% of all adults.
As the Kaiser Family Foundation's Larry Levitt just noted:
This held up. 70% of adults vaccinated by July 4th was not a low bar designed for an easy political win. And, it will still be an important goal even after July 4th passes and President Biden’s target isn’t achieved, as expected. https://t.co/J0nB9XXECu
Missouri just voted #YesOn2 to expand Medicaid, and now, because of YOUR vote, over 230,000 hardworking people will have access to life-saving healthcare!pic.twitter.com/azHN0GJjEW
— YesOn2: Healthcare for Missouri (@YesOn2MO) August 5, 2020
Republican lawmakers blocked Medicaid expansion funding from reaching the Missouri House floor on Wednesday, posing a setback for the voter-approved plan to increase eligibility for the state health care program.
The Washington Health Benefit Exchange (Exchange) reports that tens of thousands of Washingtonians now pay less each month for healthcare coverage. Within two months of the American Rescue Plan Act (ARPA) becoming federal law, the Exchange passed on the expanded savings it made available to new and current customers on the state’s insurance marketplace, Washington Healthplanfinder.
“There has never been a better time to sign up for healthcare coverage in Washington,” said Pam MacEwan, Chief Executive Officer of the Exchange. “We’ve been hearing from people across the state who are saving hundreds or in some cases more than a thousand dollars per month.”
Tracy Roberts from Seattle posted to Facebook, “I just opened my bill for July and it’s $242 less than I presently pay . . . That’s incredible! Absolutely incredible and completely unexpected. Life will be a little easier for now.”
This, again, is a Big Deal for this year. Paired with the beefed-up APTC table, what it means is that if you're on unemployment this year you effectively don't have to pay anything for a benchmark Silver plan. I'm not sure if you have to be unemployed for the full year or not...the wording above sounds like even someone who's only on unemployment for one or two weeks would still be counted as having 133% FPL.
Sure enough, just about anyone who is either currently receiving unemployment benefits or who did earlier this year (or later this year, for that matter) is likely eligible for a FREE ($0* Premium) Silver CSR 94 plan...otherwise known as #SecretPlatinum:
I should also note that not every NBPP rule implemented by the Trump Administration (via CMS Administrator Seema Verma) has been terrible. Some are either perfectly in line with Obama-era NBPPs, inconsequential, and in a few cases have actually been good and helpful.
...Other proposed changes, however, can be either stupid or flat-out devastating. The proposed 2022 rule changes...which were pushed out after hours on Thanksgiving Eve, just 56 days before the Trump Administration ends...includes some OK ideas, but also includes some which would be harmful and one which would be disastrous (I've changed the order they're listed below to put the most troubling ones at the bottom):
The details get wonky, but the bottom line is that there were three proposed rule changes in particular which I was deeply concerned about: