Believe it or not, even though Delaware is a fairly solidly blue state in Presidential elections, two of the three counties there (it's pretty small) voted for Donald Trump in 2016. Here's how the state's cases have shifted over time between New Castle County (the largest of the three, which voted for Clinton) and the other two counties which voted for Trump:
This is almost a complete reversal, with New Castle going from 2/3 of all cases at the beginning of April to just 1/3 today:
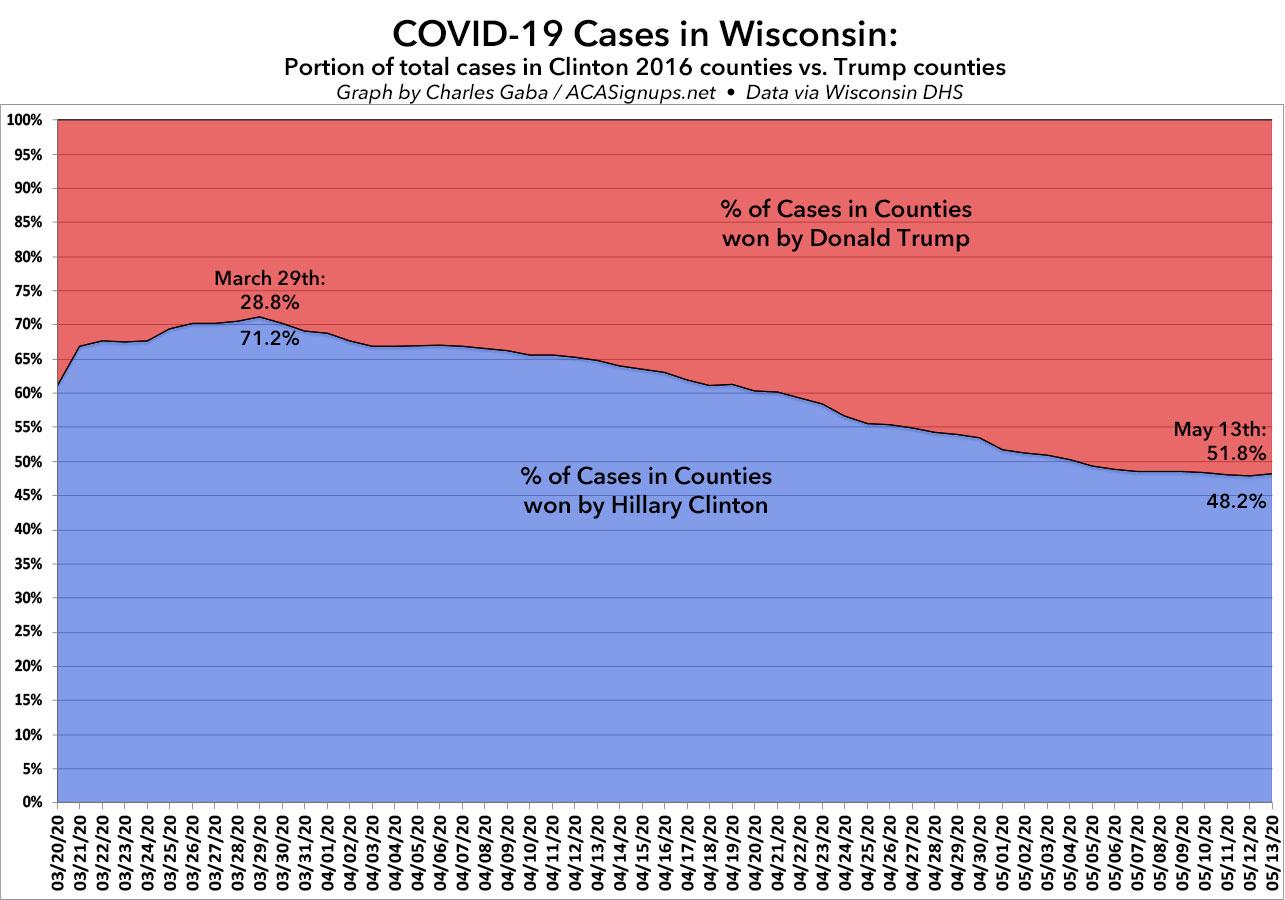
A few weeks ago, I posted a detailed analysis of how the COVID-19 virus has been spreading throughout Wisconsin. I noted that while the outbreak originally spread quickly in the more urban/blue-leaning areas, that has gradually changed over time, with the virus spreading to the rest of the state--including rural, conservative-leaning areas--at a faster rate while it slowed down in the urban areas.
It's time to check in to see whether that trend has continued...and sure enough, it has. Here's what this trend looks like visually:
A few weeks ago, I posted a detailed analysis of how the COVID-19 virus has been spreading throughout my home state of Michigan. I noted that while the outbreak originally spread quickly in Detroit and the more densely-populated Metropolitan Detroit region (Wayne, Oakland and Macomb counties), that has gradually changed over time, with the virus spreading to the rest of the state--including rural, conservative-leaning areas--at a faster rate while it slowed down in the urban areas.
It's time to check in to see whether that trend has continued...and sure enough, it has:
Due to the COVID-19 emergency, Vermont Health Connect has opened a Special Enrollment Period until May 15, 2020. During this time, any uninsured Vermonter can sign up for a Qualified Health Plan through Vermont Health Connect. Qualified families can also get financial help paying for coverage.. Please call us at 1-855-899-9600 to learn more.
More than 14,000 Coloradans gain health coverage during emergency Special Enrollment Period; Marketplace reports higher enrollments and lower costs in 2020
DENVER — A total of 14,263 Coloradans gained health insurance coverage during Connect for Health Colorado’s emergency Special Enrollment Period, which ran from March 20 to April 30. The Marketplace opened the Special Enrollment Period in response to the outbreak of the coronavirus (COVID-19), to ensure as many Coloradans as possible have access to health care.
“We’ve seen a tremendous response to the emergency Special Enrollment Period and need for affordable health coverage,” said Chief Executive Officer Kevin Patterson. “As always, we are here to help Coloradans get covered and stay covered as they navigate life changes this year.”
MNsure offers enrollment opportunity for Minnesotans newly eligible for financial help due to decrease in income
MNsure is the only place to get financial help to lower the cost of health insurance
Starting May 11, 2020, MNsure is offering an ongoing special enrollment period for Minnesotans who experience a decrease in household income and become newly eligible for advanced premium tax credits (APTC). Those looking to enroll will need to have had health insurance that meets the standards in the Affordable Care Act, also known as minimum essential coverage (MEC), for one or more days in the 60 days immediately preceding their decrease in household income.
Minnesotans must act within 60 days after they experience a decrease in household income to be eligible.
Regular readers have no doubt noticed that I've let the blog sit mostly idle for the past week or so, even though there's been a ton of noteworthy developments. As I noted on Friday, part of this was due to an emergency laptop replacement/transfer. Part of it was due to it being Mother's Day weekend. Part of it was due to some other personal issues.
This has been far more difficult than you might imagine. While there are a half a dozen great sites out there already doing up-to-date tracking of COVID-19 data at the state level, such as the COVID Tracking Project, WorldoMeters and so forth, when it comes to the county-level data, it's a very different story. Some state health department websites make this data easily available and in an easy-to-read format; others make it next to impossible.
Since tracking and analyzing data is what I'm best known for...and since I'm mostly stuck sitting in front of the computer all day whether I like it or not these days anyway...I've started my own daily COVID-19 spreadsheet.
Again, I'm not the one who compiled the data itself--many other teams with far better resources than I have are doing that--but I'm pulling their work together and adding some additional context, such as per capita info by state/territory.
You may have noticed that I haven't posted many entries the past week or so aside from nightly COVID summaries and a few reposts of SBM press releases. Two reasons for this:
First, I've been spending a lot of time expanding/updating my county-level COVID-19 spreadsheets, which I've split off onto their own link (the state-level version was starting to get bogged down...it has over 40 daily worksheets; apparently the addition of the county-level sheets was slowing it down)
Second, my 8-year old laptop had a meltdown (literally, of sorts...the battery overheated and swelled up); I had to scramble to replace it (it was overdue anyway), which wasn't easy to do on short notice in the middle of a shelter-at-home pandemic. I've been spending the week transferring over gobs of data, updating software and/or getting replacement software for incompatible versions. It's a painstaking process.
Anyway, I'm more than a little backed up and plan on catching up ASAP.
Since tracking and analyzing data is what I'm best known for...and since I'm mostly stuck sitting in front of the computer all day whether I like it or not these days anyway...I've started my own daily COVID-19 spreadsheet.
Again, I'm not the one who compiled the data itself--many other teams with far better resources than I have are doing that--but I'm pulling their work together and adding some additional context, such as per capita info by state/territory.