My county-level tracking project continues. I've now plugged in confirmed/official COVID-19 cases and fatalities across 36 states and hope to bring the remaining 14 states (plus the U.S. territories) up to date within the next few days.
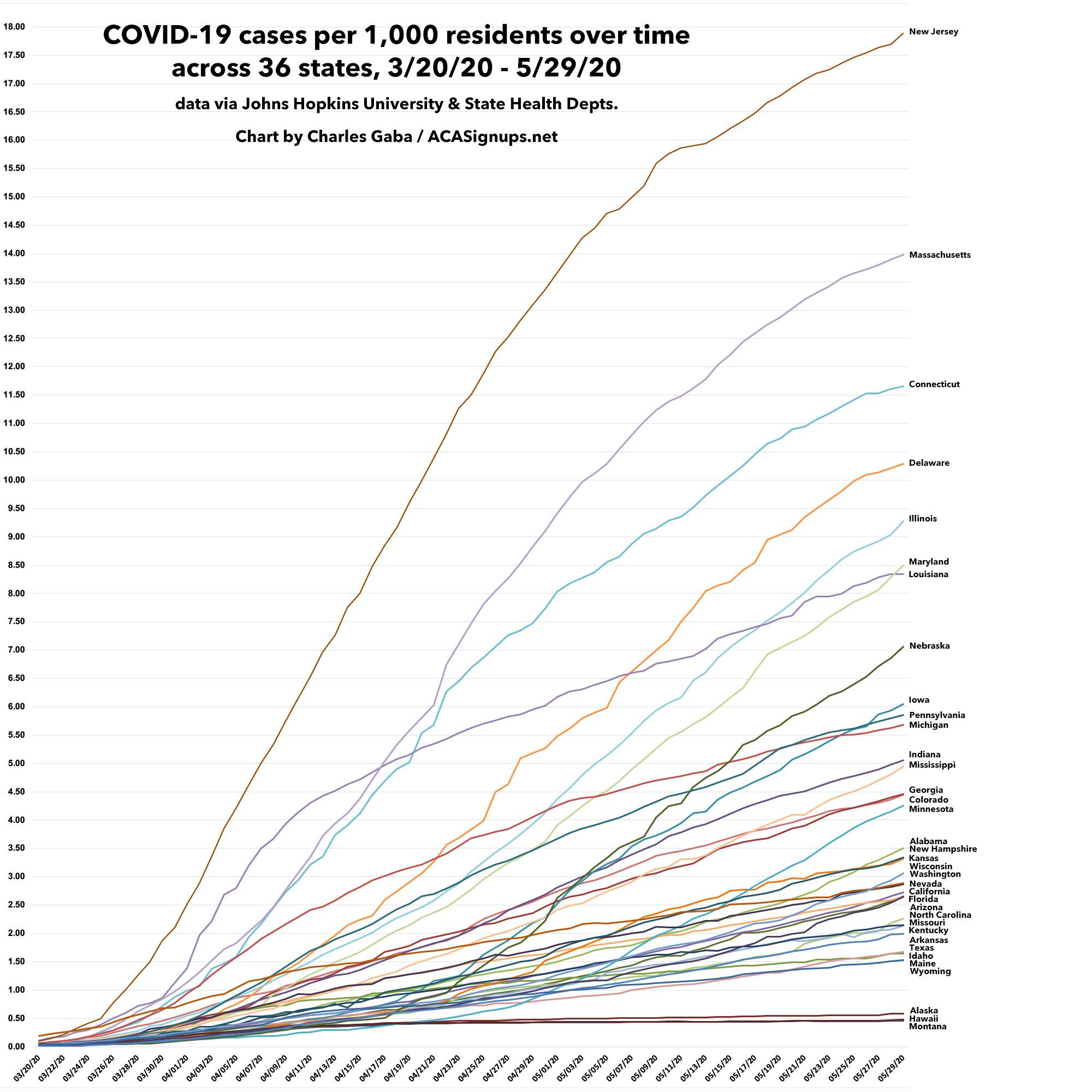
Meanwhile, here's how cases have spread on a per capita basis across those 26 states from March 20th until May 29th. At the high end, I haven't gotten to two of the worst-hit states yet (New York & Rhode Island); at the lower end, there's a cluster of states which are difficult to separate out at this level as they're running so close together.
Just as important as the infection rate itself, of course, is the curve of the line. Louisiana and Michigan were hit hard early on, but seem to be flattening their curves, while states like Minnesota, Iowa, Mississippi and Alabama, which were hit later, are starting to curve upwards now, definitely the wrong direction.
Since I've been neglecting other ACA/healthcare posts the past couple of weeks, I figured I should at least provide regular updates on why I've been mostly absent.
I've made major progress in updating and revising my breakout of COVID-19 cases and fatalities at not just the state level but the county level. Again, I've separates the states into two separate spreadsheets:
This page contains proposed health plan rate information for the District of Columbia’s health insurance marketplace, DC Health Link, for plan year 2021.
The District of Columbia Department of Insurance, Securities and Banking (DISB) received 188 proposed health insurance plan rates for review from Aetna, CareFirst BlueCross BlueShield, Kaiser Permanente and United Healthcare in advance of open enrollment for plan year 2021 on DC Health Link, the District of Columbia’s health insurance marketplace.
The four insurance companies filed proposed rates for individuals, families and small businesses for the 2021 plan year. Overall, 188 plans were filed, compared to 181 last year. The number of small group plans increased from 156 to 163, and the number of individual plans remained at 25.
In the middle of a deadly global pandemic which has already killed more than 100,000 Americans and completely disrupted the entire U.S. healthcare system, private insurance carriers still have to go about preparing their annual premium rate change filings for 2021. This is a long, complicated process which begins a good nine months before the new plans and prices are actually enrolled in.
The task of setting 2020 premiums was the first time since the ACA went into effect which was relatively calm for insurance carrier actuaries:
My county-level tracking project continues. I've now plugged in confirmed/official COVID-19 cases and fatalities across 26 states and hope to bring the remaining 24 states (plus the U.S. territories) up to date within the next few days.
Meanwhile, here's how cases have spread on a per capita basis across those 26 states from March 20th until May 23rd. At the high end, I haven't gotten to the worst-hit states yet (New York, New Jersey, Massachusetts & Rhode Island), which wouldn't fit on this chart anyway; at the lower end, once you get below Alabama, there's a cluster of states which are difficult to separate out at this level as they're running so close together.
Just as important as the infection rate itself, of course, is the curve of the line. Louisiana and Michigan were hit hard early on, but seem to be flattening their curves, while states like Minnesota, Iowa and Alabama, which were hit later, are starting to curve upwards now, definitely the wrong direction.
I've made major progress in updating and revising my breakout of COVID-19 cases and fatalities at not just the state level but the county level. Again, I've separates the states into two separate spreadsheets:
Most of the data comes from either the GitHub data repositories of either Johns Hopkins University or the New York Times. Some of the data comes directly from state health department websites.
I hope to fill in the back-data for every state within the next few days, bringing them all up to date. This should allow for plenty of interesting analysis of trends and counties to keep an eye on. It will also allow me to get back to posting more regular ACA policy updates/etc.
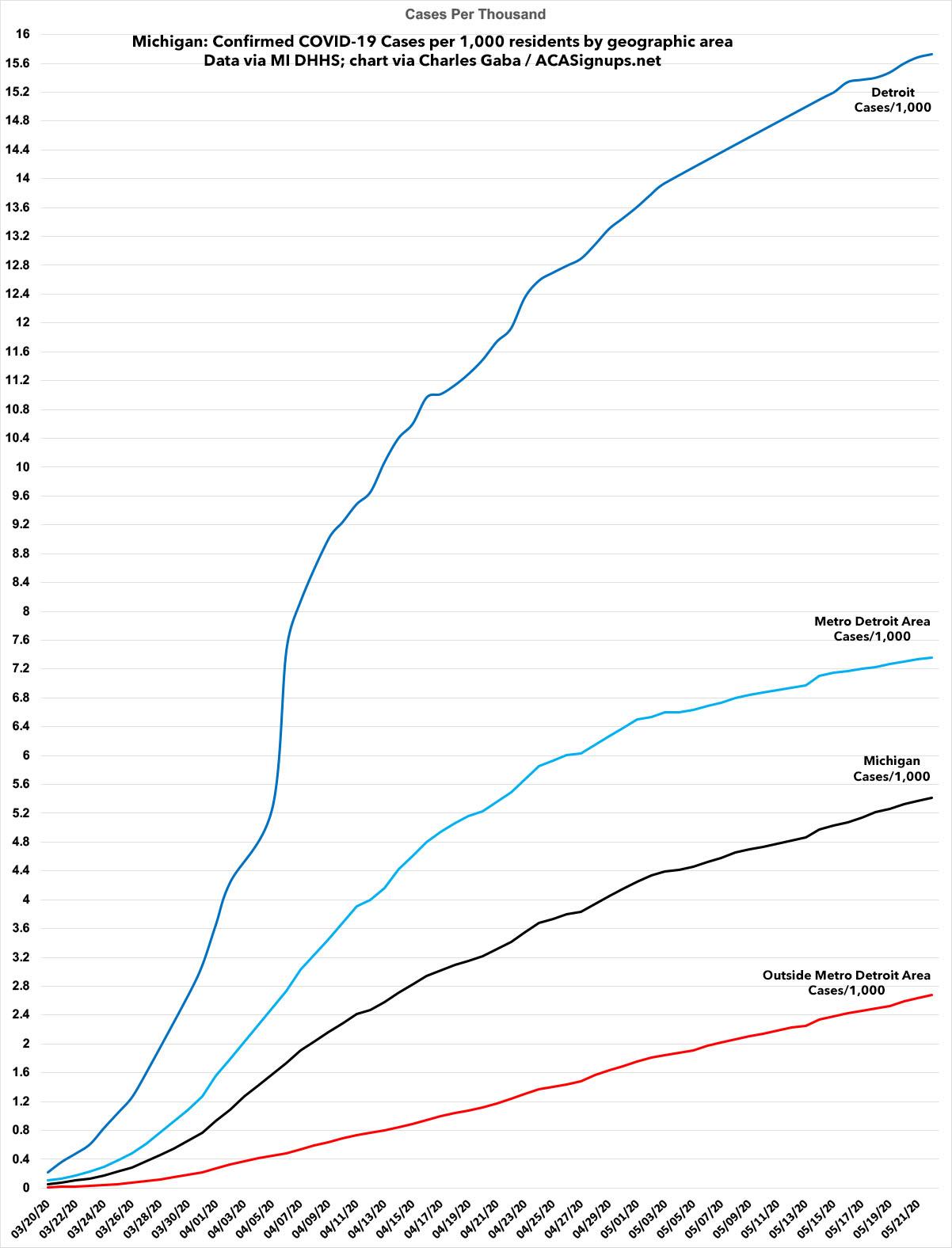
As a follow-up to my prior posts about the urban/rural divide of how COVID-19 has spread throughout Michigan, here's a graph which shows how it's spread in Detroit, the larger Metro Detroit area and the rest of the state on a per capita basis over time.
Obviously the probem is still far worse in Detroit and the Metro Detroit area overall...but the case trendlines are starting to flatten in Detroit and Metro Detroit, while it's still increasing at the same rate or higher in the rest of the state.
Massachusetts Health Connector continues extended enrollment as nearly 45,000 people enroll in new plans, update current coverage
April 28, 2020 – The Massachusetts Health Connector continues to help people who need health insurance after losing coverage or income due to the coronavirus, with a May 23 deadline ahead for June 1 coverage.
Silver State Health Insurance Exchange enrolls 5,479 during Exceptional Circumstance Special Enrollment Period in Response to COVID-19
Carson City, Nev. – The Silver State Health Insurance Exchange (Exchange), Nevada’s state agency that helps individuals secure budget-appropriate health coverage through the online marketplace and State Based Exchange (SBE) platform, Nevada Health Link, enrolled 6,017 Nevadans during its limited-time Exceptional Circumstance Special Enrollment Period (SEP), March 17 – May 15, including 5,479 new consumer enrollments related to the Exceptional Circumstance Special Enrollment Period, and 538 enrollments due to loss of Minimum Essential Coverage (MEC).
In response to Governor Sisolak’s March 12 Emergency Declaration, the SEP was opened to allow qualified Nevadans who missed OEP to secure health care coverage. Consumers who enrolled on or before April 30 received coverage effective May 1, and consumers who enrolled between May 1 and 15 will have coverage effective June 1, 2020.