For 2017, unsubsidized enrollees on the Minnesota individual market faced massive rate hikes averaging 57%. It was so bad that the only way they could convince some carriers to participate in the market was to allow most of them to put a cap on how many people they'd enroll (with the balance being shunted over to Blue Plus, the HMO division of BCBSMN). This resulted in a massive initial surge of enrollment, as it was on a first-come, first-serve basis...but also left off-exchange and unsubsidized exchange enrollees high and dry.
In response, the state scrambled to pull together a $300 million package to help supplement premiums for those folks...knocking a flat 25% off of their premiums for 2017. This helped ease the problem in the short term, but the larger issue still loomed going forward.
It feels almost silly for me to spend so much time crunching the average 2018 rate hike numbers at this point. Between the (supposedly failed?) GOP repeal effort and Donald Trump's ongoing sabotage efforts--including what could be him officially pulling the plug on CSR reimbursements as early as sometime today--it's probably a bit of a futile effort. Besides, a dozen other wonks/analyses have already confirmed what the Kaiser Family Foundation projected months ago and which I've been proving on a state-by-state basis for months now: The CSR threat is causing average rate hikes of around 20 points on average, and the threats to individual mandate enforcement are tacking on another 4-5 points on top of that, beyond the ~10 points which rates would normally be increasing on average.
UPDATE 9/27/17: It now looks extremely likely that CSR reimbursement payments will not be guaranteed for 2018 (they may or may not be paid, mind you, but it's unlikely that they'll be legislatively appropriated, which amounts to the same thing as far as most insurance carriers are concerned). With this in mind, I'm re-upping this rather wonky/in-the-weeds tutorial about the #SilverSwitcharoo, since it looks like at least 6 states (California, Connecticut, Florida, Idaho, North Carolina and Pennsylvania) are likely to end up using it this fall.
UPDATE 10/12/17: Welp. Sure enough, Donald Trump is indeed officially planning on pulling the plug on CSR reimbursement payments. Several healthcare wonks, including myself, have been tracking how different states are handling the CSR load issue; so far it looks like 22 are "Silver Loading" and 10 are going "full Silver Switcharoo". This may change over the next week or so, however.
The states we know (or at least are pretty certain) are Silver Switcharooing are: California, Connecticut, Florida, Georgia*, Hawaii, Idaho, Minnesota, Nevada, South Carolina and Washington State.
*(At least one carrier in Georgia)
(Special thanks to folks like Josh Schultz, David Anderson, Andrew Sprung, Amy Lotven, Wesley Sanders and others for helping me make heads or tails out of the CSR brouhaha)
It was pretty crude, but I was scrambling to upload it ahead of the big Senate repeal/replace vote...and frankly, I felt a little silly bothering afterwards, since there was a very good chance that none of this would matter soon anyway.
Fortunately, late last night, something unexpected happened...and it now appears that the ACA will indeed live on for awhile, albeit still with serious issues to work out.
Those were Democratic Senate Minority Leader Chuck Schumer's words tonight in response to Republican Senate Majority Leader Mitch McConnell's claims that those on the left were "celebrating" the defeat of his Godawful "Skinny Repeal" bill late Thursday night. And that's a perfect description of how I feel, for several reasons:
1. This wasn't so much a case of an "Actively Positive" thing happening (as was the case with, say, the Obergefell v. Hodges Supreme Court decision) as it was stopping a negative thing (as was the case with the King v. Burwell SCOTUS decision, which actually was announced the very same day as Obergefell). That is to say, it's not that a good piece of legislation passed, it's that a bad piece of legislation was blocked. This isn't to minimize the importance of what just happened tonight (not just in terms of healthcare policy, but also the state of our democratic process, legislative norms and of course the ramifications for the rest of this ongoing nightmare we call the Trump Administration), but it does tend to dampen my emotional response a bit.
2. As I keep stressing: There are real problems with the ACA as it currently stands, and some of them require more than simple "tweaks" as some ACA defenders are prone towards describing them. All of these problems are definitely fixable, but most of those solutions still won't be easy to push through. Furthermore, these issues are exacerbated by two other problems:
3. THE CLOCK IS TICKING for 2018: The final carrier rate filing deadline is rapidly approaching; the carriers need to make their final decisions about how much to charge next year soon...assuming they decide to stick around the individual market next year at all, which isn't a guaranteed thing, especially due to...
4. THE TRUMP SABOTAGE FACTOR will now almost certainly go into overdrive. I'm about 90% certain that Trump will indeed pull the plug on Cost Sharing Reduction reimbursement payments staring next month (August), which could still devastate the indy market almost instantly. Of course, Congressional Republicans could resolve the CSR issue in about 5 minutes with a simple, 87-word bill which would receive unanimous consent from every Democrat in both the House and Senate as long as it was either standalone or not attached to some other poison pill piece of legislation.
For that matter, while the individual mandate repeal died with the "Skinny Repeal" bill failing, House Republicans have also started pushing through a different bill which would prevent the IRS from enforcing the individual mandate anyway, causing the exact same problems. And even if that doesn't happen, HHS Sec. Tom Price could simply start issuing hundreds of thousands of highly-questionable "hardship exemptions" letting pretty much everyone off the hook for the mandate penalty anyway...which, once again, would amount to the same fallout.
For the past six months, I've been giving a PowerPoint presentation to various activist clubs/meetings around Southeast Michigan about the Affordable Care Act and Republican attempts to repeal it, including the basics of how the ACA was supposed to work, which parts are and aren't working (and why), how I'd recommend fixing the real problems and, of course, just what the heck the GOP has been trying to do to tear it all apart.
Many people have requested an online version of the slideshow. I posted an earlier version of it this past spring, but obviously things have changed dramatically over the past few months.
I've updated and enhanced about 3/4 of the slideshow. Unfortunately, I haven't had a chance to update the GOP repeal section yet--it's sort of a mish-mash of AHCA and BCRA slides right now, but I thought it was more important to get it posted for the moment under the circumstances.
Then again, that section keeps changing every five minues anyway, so perhaps it's just as well if I hold off on that part. I'll swap out this version for a newer one at a later date.
(yes, I know she actually says "bumpy night"...I'll update the title this evening if need be...)
OK...here's where things stood as of last night...
UPDATE 7/27/17 12:00pm: OK, here's the latest (at least, as of around noon, anyway):
Apparently, in order to win over a few more votes and squeeze the bill in under the "budget savings" wire, they're now planning on scrapping repeal of the medical device tax and delaying repeal of the employer mandate (but still repealing it eventually). They're also going to throw in defunding Planned Parenthood even though that was previously scrapped by the Senate parlimentarian.
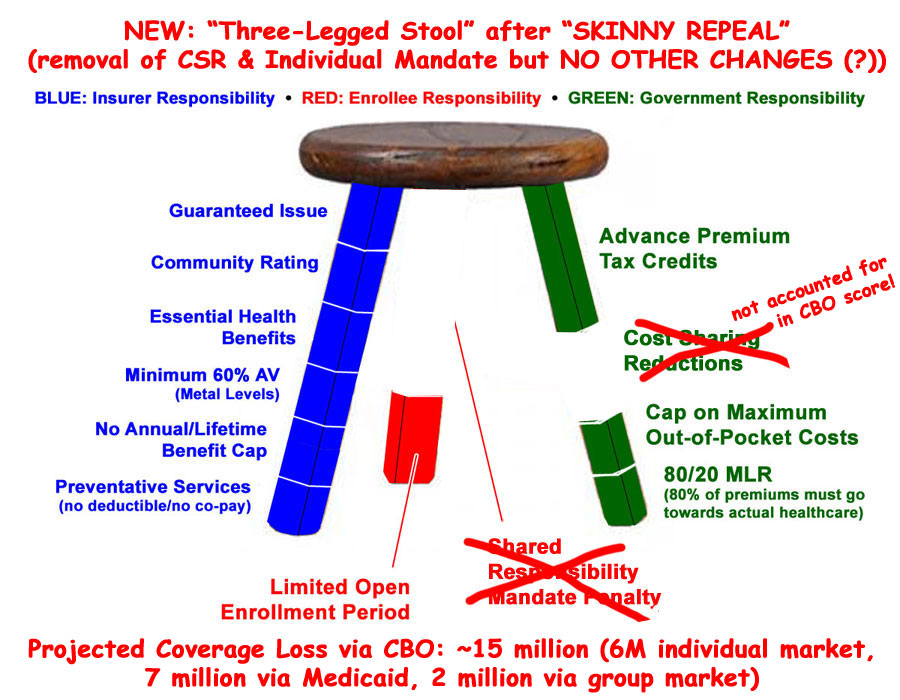
Finally, they're apparently bringing back theEssential Health Benefit State Waiver provision, which would, once again, blow a massive hole in the "Guaranteed Issue and Community Rating" rules.
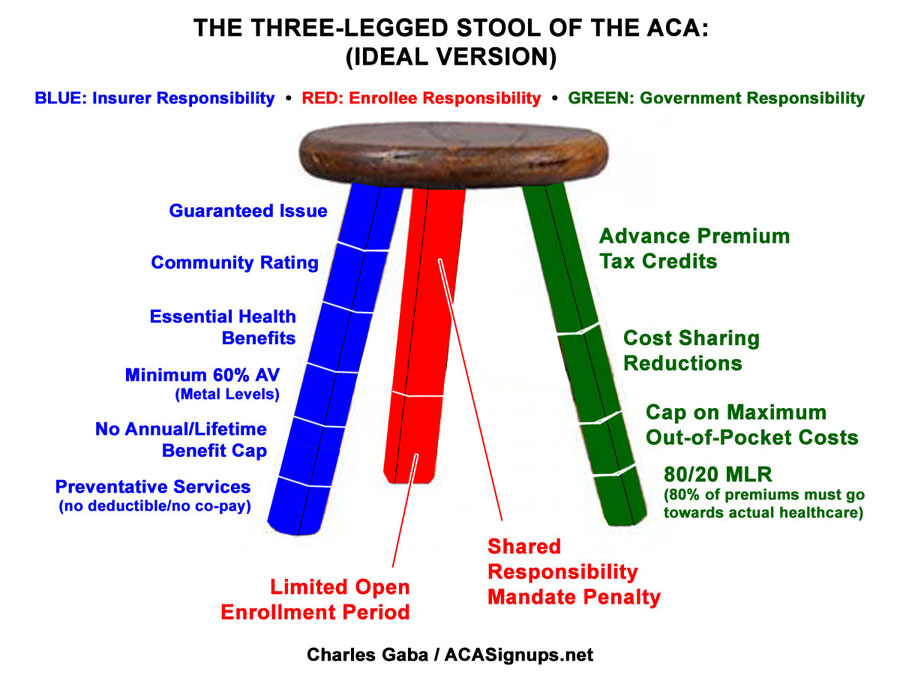
UPDATE: Hey, who's that up there? Why it's the guy who Republicans wanted to become President just 5 years ago, explaining why, if you're going to guarantee solid health insurance policies to everyone regardless of their medical history and without discriminating on price, you have to include some sort of incentive for them to do so: A carrot and a stick. The tax credits and out of pocket maximums are the carrot. The individual mandate and open enrollment period are the stick.
(sigh) I debated whether to even write a post about the last-minute "Skinny Repeal" plan slapped together by Mitch McConnell yesterday morning for a couple of reasons: First, because even if it passes, the sole purpose of "Skinny Repeal" is to get past the 50-vote Senate threshold...at which point it would be scrapped and replaced with whatever Godawful pile of garbage McConnell comes up with via reconciliation afterwards anyway.
Second, and more to the point, they're supposed to be voting on "Skinny Repeal" within the next few hours, so it's possible that it could be a moot point before anyone even reads this.
OK. Here we go. First, just as a refresher: Here's what the Individual Market was supposed to look like under the Affordable Care Act:
Here's what it actually looks like for a variety of reasons, including both legitimate glitches in the ACA itself as well as a whole lot of flat-out sabotage by the GOP over the past 7 years. While there are plenty of other issues which need to be addressed, the most obvious ones are that the tax credits need to be beefed up and applied to enrollees over the 400% FPL threshold, and the mandate penalty should really be increased. In short, two legs of the stool need to be lengthened...to continue the metaphor, we need a couple of shims. Around $12 billion per year or so should do the trick on the tax credit side. As it happens, one of the few useful parts of most of the GOP plans is that they do include a good $120 billion or so in "reinsurance/stabilization" funding over 10 years...which, in practice, would amount to about the same thing. The key is that this funding would have to be added to the existing ACA funding, not replacing it, which is what these plans do instead: