Last week I noted that Ted Cruz's proposed amendment to the GOP Senate's BCRAP bill is a big pile of crap all by itself, since it would effectively turn the ACA-compliant market into a massively underfunded High Risk Pool, while likely turning the non-compliant individual market into a wasteland of subprime junk insurance (or at best, plans which are reasonable right up until you get truly sick, in which case you're screwed).
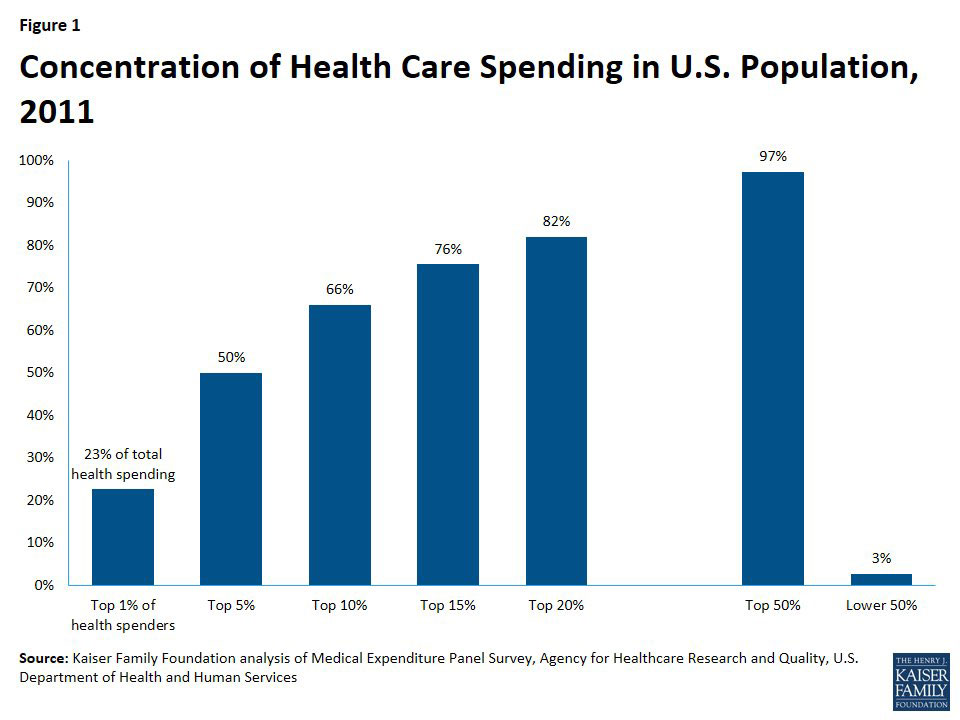
To help explain how this would happen, I used this bar graph from the Kaiser Family Foundation to show how medical expenses are actually split up by different subsets of the population:
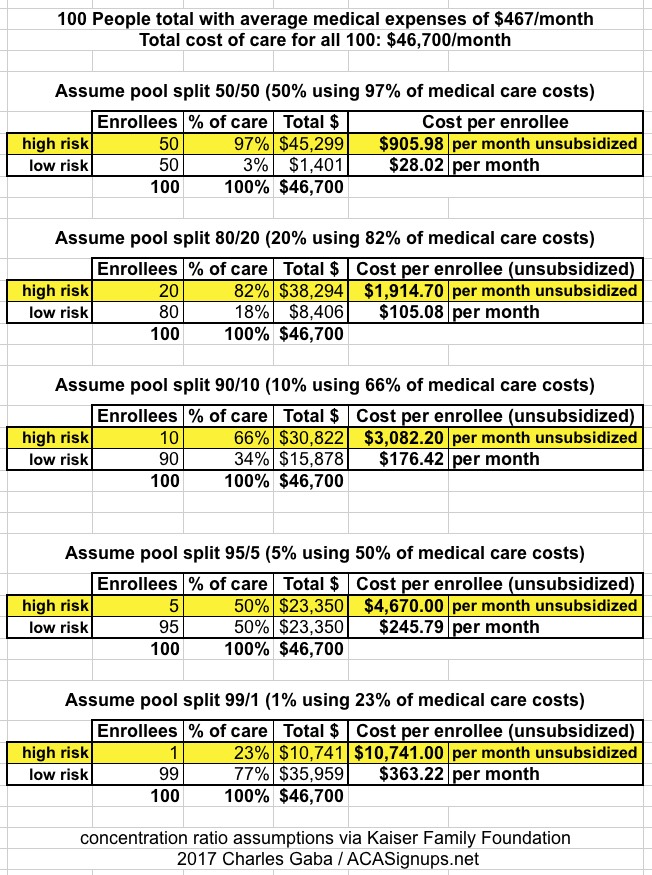
Based on these averages, I put together several scenarios showing what typical premiums might be for "ACA Enrollees" and "Cruz Enrollees" depending on how the market was split up:
Senate Majority Leader Mitch McConnell (R-KY) announced Tuesday that he is canceling half of Congress’ annual month-long August recess, keeping lawmakers in town to finish their drawn-out and so far unsuccessful effort to repeal the Affordable Care Act and tackle other pressing matters.
“Once the Senate completes its work on health care reform, we will turn to other important issues including the National Defense Authorization Act and the backlog of critical nominations,” he wrote.
Tensions are rising between Senate Majority Leader Mitch McConnell’s leadership team and his party’s ideological factions, with a renewed sense of pessimism creeping into the Senate GOP’s efforts to repeal Obamacare.
Fewer issuers apply to participate in Health Insurance Exchanges for 2018
Fewer issuers apply to participate in Health Insurance Exchanges for 2018
Less choice for consumers as issuer health plan applications drop 38 percent from last year
The Centers for Medicare & Medicaid Services (CMS) today announced 141 individual market qualified health plan (QHP) issuers submitted initial applications to offer coverage using the Federally-facilitated Exchange eligibility and enrollment platform in 2018. At the initial filing deadline last year, 227 issuers submitted an application compared to 141 this year, a 38 percent drop in filings.
For months now, I've been noting that multiple analyses by the CBO, S&P and others kept agreeing that as ugly as 2017's average unsubsidized rate hikes were (around 25% overall nationally, ranging from just 1.3% in Rhode Island and North Dakota to a whopping 76% in Oklahoma), they did appear to do the trick in terms of finally bringing individual market premiums in line with actual medical expense claims, thus stabilizing the overall risk pool. Yes, there are still many areas of the country where this isn't the case yet, but overall it looked like the dust had finally started to settle, allowing a clear picture of what needs to be done next to improve the situation.
Rhode Island just released their 2018 Individual and Small Group market rate hike requests, and they're pretty straightforward. For the small group market, I don't have the weighted market share for each carrier, but overall it ranges from 5.8 - 12.8%, with an unweighted average of 8.8%.
On the individual market, as with 2017, there's only two carriers participating in 2018: BCBS of RI and Neighborhood Health Plan. They're asking for a 13.8% and 5.0% increase respectively, with a weighted average of 10.5%.
BCBS gave their enrollment as around 27,000; for Neighborhood, I estimated theirs based on dividing their projected total member months by 12 to get 16,345. RI's on-exchange enrolment was 29,456 during Open Enrollment this year, so that would leave roughly 12,800 off-exhange enrollees, for roughly a 2:1 on/off-exchange ratio, which sounds about right.
Including Georgia, I've now compiled initial 2018 unsubsidized individual market rate hike requests for 17 states...and Georgia's carriers are asking for by far the highest overall average increase, even assuming no Trump/GOP sabotage tax.
There appear to be four carriers which have filed to sell individual market plans in Georgia next year: Alliant, Ambetter (aka Celtic, aka Centene...for God's sake, pick one name, guys, willya??), Anthem Blue Cross Blue Shield and Kaiser Health Plan.
New data have been released contradicting Republican propaganda about the “failing” Affordable Care Act. What may be more embarrassing to the hardliners pushing repeal is that it comes from the government, specifically the Department of Health and Human Services.
Under Secretary Tom Price, the department has been a fount of anti-ACA rhetoric. But in an annual report about the ACA’s risk-management provisions issued Friday, Health and Human Services established that the key programs are “working as intended,” protecting insurers from unexpectedly large risks and moderating premiums for consumers.
Not only that, the data “would seem to refute the commonly held belief that the marketplace population is becoming sicker,” observes health economist Timothy Jost, writing in Health Affairs. In fact, according to the figures from 2016 in the latest report, the customer base is getting healthier and the risk pools have been stabilizing.
His proposal, which he’s circulating to his colleagues on typed handouts, wouldn’t explicitly create and fund the special insurance markets, as the House bill did. Instead, insurance experts said, it would create a sort of de facto high risk pool, by encouraging customers with health problems to buy insurance in one market and those without illnesses to buy it in another.
...There is no public legislative language yet, but here’s how Mr. Cruz’s plan appears to work, based on his handout and statements: Any company that wanted to sell health insurance would be required to offer one plan that adhered to all the Obamacare rules, including its requirement that every customer be charged the same price. People would be eligible for government subsidies to help buy such plans, up to a certain level of income. But the companies would also be free to offer any other type of insurance they wanted, freed from Obamacare’s rules.
At the top of the website I have a button linking to an article I wrote for Cracked.com back in May in which I explored about a half-dozen reasons why making major changes to healthcare policy in the U.S. is such a royal pain in the ass. I'm a Single Payer advocate at heart, so it was mostly written from that perspective, but really, most of the points I made would apply to any major policy change.
One thing you may notice in reading the piece is that at no point do I address the cost/payment side of moving the entire U.S. over to a universal, federally-funded Single Payer system; I stick mostly to the logistical side of things (What to do with 2-3 million industry workers? What about the Hyde Amendment? Etc, etc). These are all reasons why I'm convinced that achieving such a system would have to be done in stages. That doesn't mean tiny stages, mind you; "incremental" simply means "more than one step", so it could be, say, 4-5 stages phased in over 20 years or whatever...just not all in one shot.
As longtime readers know, I've often separated the problems with the ACA into several categories:
Some were inherent in the original bill as signed into law.
Yes, many of these only exist because of futile attempts to win over support from Republicans (or a handful of blue dog Dems), but the Democrats are still responsible for them. This includes things like the APTC tax credits being too skimpy, the "family glitch", the "skinny ESI glitch" and so forth. In these cases, the GOP can certainly be criticized for refusing to help resolve those issues, but that's a matter of "passive" obstruction as opposed to overtly doing so.