New Reports Show Record 35 Million People Enrolled in Coverage Related to the Affordable Care Act, with Historic 21 Million People Enrolled in Medicaid Expansion Coverage
Last June, the U.S. Health & Human Services Dept. confirmed my estimate that total enrollment in healthcare policies either specifically created by (or expanded to more people by) the Affordable Care Act had broken 31 million Americans:
Today, the U.S. Department of Health and Human Services (HHS) released a new report that shows 31 million Americans have health coverage through the Affordable Care Act – a record. The report also shows that there have been reductions in uninsurance rates in every state in the country since the law’s coverage expansions took effect. People served by the health Marketplaces and Medicaid expansion have reached record highs.
That would put the national final QHP total at somewhere between 12.9 - 13.2 million people nationally as of January 31st, 2022; call it around 13.1 million.
...I completely forgot to mention BASIC HEALTH PLAN (BHP) enrollment in New York and Minnesota. It totalled 975,337 people during the 2021 OEP (883,451 in New York, 91,886 in Minnesota)...I'm willing to bet total BHP enrollment across both states will end up perhaps 10% higher year over year, which would put it at around 1.1 million.
When you add that to my QHP projection above, you get a grand total of perhaps 14.1 million QHPs + BHPs combined.
If this projection had proven accurate, it would have meant total ACA exchange enrollment was up ~9 - 10% year over year, which would have been impressive but not stellar.
Now that we have two weeks worth of 2022 Open Enrollment data under our belt (well...for 33 states, anyway), I thought this would be a good time for me to try and put together a spitball estimate of how many Americans are likely to enroll in ACA exchange coverage during the 2022 Open Enrollment Period (OEP).
There's really two main numbers to try and project: How many current enrollees will renew/re-enroll for 2022 (whether actively or automatically); and how many new enrollees will jump into the ACA exchanges?
For each of these, due to how the data is reported, I have to further break the states out between those using the federal ACA exchange (HealthCare.Gov) and those which operate their own state-based ACA exchanges (Covered California, NY State of Health, etc.) This is further complicated by the fact that three states (Kentucky, Maine and New Mexico) switched from the federal exchange to their own state-based exchange starting with the 2022 OEP.
Not too many changes were made in either market. I get a weighted average increase of 4.6% for individual market plans (MI DIFS puts it at 4.7%), while I get exactly +7.0% for small group plans (MI DIFS puts it at +7.1%).
As I noted in August, the other noteworthy changes are:
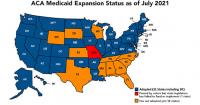
They also estimate that another 1.8 million uninsured Americans who are eligible for subsidized ACA exchange plans who would be eligible for Medicaid instead if those state actually did expand Medicaid (and perhaps another 100K in Missouri). That's nearly 4.0 million total...
So, how to crack this nut in these holdout states, all of which are either completely or partially controlled by Republicans who have adamantly refused to expand the program no matter what all these years?
Highlighting Michigan’s increasingly competitive health insurance market, the Michigan Department of Insurance and Financial Services (DIFS) has reported that consumers will have more health plan options from an increased number of insurers on the Health Insurance Marketplace for the upcoming open enrollment period.
“As we look toward the end of the pandemic and beyond, it is critical that Michiganders are able to get the affordable, high quality health coverage they need for themselves and their families,” said DIFS Director Anita Fox. “Consumers will have more options to choose from when shopping for health insurance coverage on the Marketplace during open enrollment later this year.”
HHS Encourages States to Educate Eligible Immigrants about Medicaid Coverage
Today, the US Department of Health and Human Services (HHS), through the Centers for Medicare & Medicaid Services (CMS) issued an informational bulletin to states’ Medicaid and Children’s Health Insurance Program (CHIP) agencies reaffirming that the 2019 Public Charge Final Rule – “Inadmissibility on Public Charge Grounds” – is no longer in effect and states should encourage their eligible immigrant populations to access public benefits related to health and housing.
Missouri just voted #YesOn2 to expand Medicaid, and now, because of YOUR vote, over 230,000 hardworking people will have access to life-saving healthcare!pic.twitter.com/azHN0GJjEW
— YesOn2: Healthcare for Missouri (@YesOn2MO) August 5, 2020
Republican lawmakers blocked Medicaid expansion funding from reaching the Missouri House floor on Wednesday, posing a setback for the voter-approved plan to increase eligibility for the state health care program.
As I (and others) have written many times, closing the so-called "Medicaid Gap" is one of the trickiest challenges President Biden and Congressional Democrats face when it comes to strengthening and improving the Affordable Care Act.
Once again: Under the ACA, all Americans earning up to 138% of the Federal Poverty Level (FPL)... roughly $17,700/year for a single adult or around $36,500 for a family of four...were supposed to be eligible to join Medicaid regardless of their health status, whether they had kids and so forth.
This was supposed to be the case in all 50 states and the District of Columbia (I'm not sure about Puerto Rico or the other U.S. territories...many ACA provisions never applied to them in the first place).
Unfortunately, one of the major consequences of the NFIB vs. Sebelius Supreme Court Case in 2012 was that expansion of the Medicaid program has to be voluntary on the part of each state.