The Washington Health Benefit Exchange today released its Spring Health Coverage Enrollment Report detailing the more than 1.6 million customers – one in four Washingtonians – who used Washington Healthplanfinder to access their 2019 health insurance coverage.
Nearly 200,000 customers used the state’s online marketplace to purchase a Qualified Health Plan (QHP) for coverage this year, adding to the more than 1.4 million residents who connected with free or low-cost health insurance through Washington Apple Health. In several rural counties (Adams, Grant, Okanogan, Pacific and Yakima), nearly half of the population relied on Washington Healthplanfinder to enroll in a 2019 health insurance plan.
When I first watched the video, I got hung up on a different aspect of Alec Smith's story...the question of whether or not he would have qualified for tax credits via an ACA exchange policy based on his income. I reached out to Alec Smith's mother, Nicole Smith-Holt, to clarify a few things from her story, but hadn't heard back yet as of yesterday morning...and made a poor decision to post the article yesterday anyway, in which I speculated, based on the limited information in the video, that Alec may have qualified for some level of assistance after all without realizing it.
The whole post was, quite simply, wrong. It was wrong for several reasons, and I'm sorry for each of them.
I laid out several of the obvious ways in which my original post was out of line, thoughtless and showed a lack of compassion. I apologized personally to Ms. Smith-Holt, she accepted, and we had a lengthy online discussion about her son's story and what led to his death:
NOTE: Julia A. Pulver, RN, BSN, CCM has been an registered nurse for over 12 years who has spent her career working with the most at risk populations in Southeast Michigan, and is also a personal friend of mine.
UPDATED with my personal initial thoughts (see below):
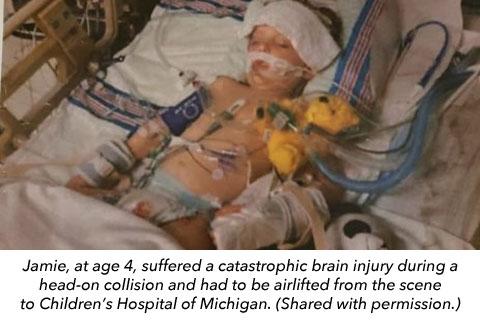
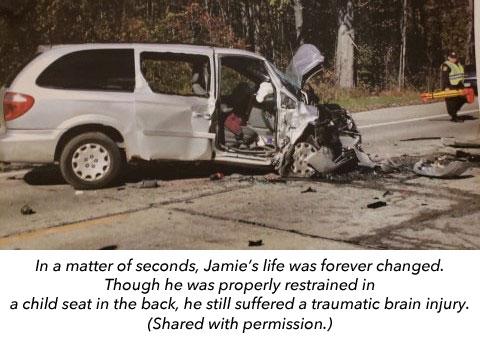
A few weeks ago I noted that Michigan Republicans were pushing hard for new Democratic Governor Gretchen Whitmer to basically eliminate Michigan's unique unlimited catastrophic care requirement for no-fault auto insurance, which is the main reason our state has the highest auto insurance premiums in the country.
Whitmer and legislative Democrats don't want people to be stuck with massive auto injury medical claims, of course, and they also wanted a guarantee of significant rate reductions as well as the elimination of "redlining" (basing rates on zip codes) and other discriminatory auto insurance pricing practices, like basing premiums on credit ratings, gender and the like.
HARTFORD, CT — Democratic gubernatorial candidate Ned Lamont has much lower expectations for what he’s going to be able to do to improve the health of Connecticut residents than one might expect from a Democratic candidate this year.
Sounds like Lamont would not push for CT to reinstate the ACA individual mandate penalty:
...Does he believe everyone in Connecticut has to purchase health insurance now that it’s not mandated by the federal government?
For a good six months or so from the fall 2017 to spring 2018, retiring Republican Senator Lamar Alexander and Democratic Senator Patty Murray tried to hash out a deal which would have, had it actually been passed and signed into law, resolved some (not all) of the ACA's stabilization issues...although at a pretty ugly cost:
Reinsurance: GOOD!
Guaranteed Ad/Outreach Funding: Good! (but only necessary due to Trump cutting funding in first place)
Short-Term Plan Notifications: Good! (but only necessary because of #ShortAssPlan EO in first place)
The Fifth Circuit just officially calendared the argument for the afternoon of July 9th. Here’s the docket entry:
CASE CALENDARED for oral argument on Tuesday, 07/09/2019 in New Orleans in the West Courtroom -- PM session. In accordance with our policy, lead counsel only will receive via email at a later date a copy of the court's docket and an acknowledgment form. All other counsel of record should monitor the court's website for the posting of the oral argument calendars.. [19-10011] (SME) [Entered: 05/23/2019 11:08 AM]
While I have you, I’m attaching the excellent reply briefs filed yesterday by the growing coalition of ACA defender states led by California Attorney General Xavier Becerra as well as the brief from the U.S. House of Representatives. Both completely take apart every single one of the absurd legal arguments put forward by the Trump-Barr DOJ and Texas et al.
With the idiotic #TexasFoldEm lawsuit scheduled for oral arguments by the 5th Circuit Court of Appeals this summer, many states have been scrambling to replicate ACA protections for those with pre-existing conditions at the state level, including California, Colorado, Connecticut, Hawaii, Maryland, Nevada, New Mexico and more.
In a red state like Louisiana, unfortunately, it's not so easy...the state has a Democratic Governor, but both the state House and Senate are solidly controlled by Republicans. In addition, the Governor, John Bel Edwards, is up for re-election this November, making everything politicized, thus making it likely impossible to get anything useful through this year. Still, Gov. Edwards is trying to do something to mitigate the problem:
The numbers are all fairly small, of course, but a few noteworthy items: DC appears to have an 89% QHP enrollment retention rate as of May from the beginning of the year (they had 18,035 QHP selections as of 1/31/19), which is very good. SHOP enrollment is disproportionately high as always for DC, due to both the fact that they require all small business enrollments in the District to be handled via the exchange and the fact that members of Congress and their staff have to use the DC exchange to enroll in healthcare coverage.
Vermont Health Connect, the VT ACA exchange, doesn't post data reports very often, but they just did so, with enrollment data as of March 2019.
It's important to note that the numbers posted in the tables below include both Vermont's on and off-exchange enrollees in the individual and small group markets. It's also important to note that Vermont (like Massachusetts) merges both the individual and small group markets into the same risk pool for purposes of premium rate settings.
There are four tables...two for the Individual market (raw numbers and percentages) and two for the small group market. Perhaps the most noteworthy line is the "Reflective Silver" enrollments...those are people who took up the "Silver Switcharoo"...basically, unsubsidized individual market enrollees who switched from (or chose) on-exchange Silver plans to off-exchange Silver plans to save money on policies which are identical to the on-exchange Silver version but without the CSR premium load.