Last week I reposted a press release & video from the Rhode Island Dept. of Administration explaining the details of a major security breach of the state's social services system.
Today it looks like the issue was a lot worse than I thought. via WPRI:
On Monday, Gov. Dan McKee said his team has identified 650,000 people whose personal information was stolen in the recent cyberattack on the state’s IT system for social services.
Yikes. FWIW, Rhode Island only has around 1.1 million people, so this basically means that 60% of the entire state population has had their personal info compromised.
...Earlier this month, the cyberattack shut down the state’s IT system known as RIBridges, which serves as an eligibility database for a host of social services, such as SNAP and Medicaid, along with subsidized health insurance through HealthSourceRI.
With Open Enrollment going on now through Nevada’s official health insurance marketplace known as NevadaHealthLink.com, there are less than two weeks left for Nevadans to get coverage starting the first of the new year. Nevadans must enroll in a plan by 11:59 p.m. on December 31, 2024, for their health insurance coverage to be effective starting January 1, 2025.
Those who don’t enroll by December 31 will still have a chance to enroll in coverage through January 15, 2025, however, those who enroll between January 1 and January 15, 2025, will have coverage beginning February 1, 2025.
Open Enrollment began on November 1 and since then, over 30,000 Nevadans have actively enrolled in a plan, with 15,236 being new to enroll on Nevada Health Link. The Open Enrollment Period is the only time of year Nevadans can freely enroll in a health insurance plan through NevadaHealthLink.com without experiencing a qualifying life event, such as getting married, having a baby or moving.
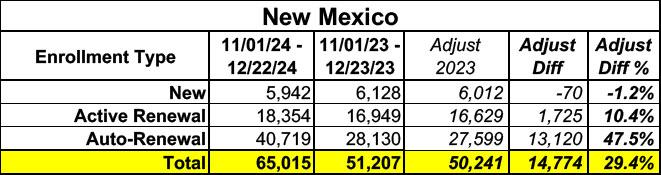
Not only is New Mexico's exchange enrollment up a whopping 29% vs. the same point last year, it's actually already 15% higher than the 2024 OEP's final total of 56,472!
Now that the two largest ACA marketplaces (HealthCare.Gov, which hosts 31 states, and Covered California) have joined a half-dozen other states in posting fairly recent 2025 Open Enrollment Period updates, I figured it would be a good time to take a look at where things stand ahead of the big holiday break.
Across 38 states, a total of around 19.5 million people have selected Qualified Health Plans (QHPs) via either the federal or state-based exchanges as of anywhere from 12/05 - 12/18. Collectively, this is roughly 16.6% higher than the same/nearly the same dates a year ago. It's important to remember that Georgia moved from the federal exchange to its own state-based marketplace this year, which is why ~1.2 million enrollees have been subtracted from the 2024 HC.gov total. Note that the HC.gov numbers are rounded off to the nearest 100K, per CMS's press releases both years.
Covered California Hits Record Enrollment Before its First Key Open Enrollment Deadline on Dec. 31
SACRAMENTO, Calif. — Covered California has surpassed 1.8 million enrollees, reaching its record-high enrollment with over a week until the first open enrollment deadline on Dec. 31.
This open enrollment, 143,686 Californians have signed up for 2025 coverage as of Dec. 14, marking a 3 percent increase over the same period last year.
Another 1,647,162 Californians have renewed their coverage so far, a 4 percent increase over the same period last year.
Combined, that's 1,790,848 Californians who have selected ACA exchange coverage for 2025. Taking the percents above literally that would mean CA had ~1,723,311 QHP selections thru 12/14/23 last year (up 3.9% overall).
Under the Inflation Reduction Act, some people with Medicare will pay less for some Part B drugs because the drug’s price increased faster than the rate of inflation.
The U.S. Department of Health and Human Services (HHS), through the Centers for Medicare & Medicaid Services (CMS), today announced that some Medicare enrollees will pay less for 64 drugs available through Medicare Part B. The drugs will have a lowered Part B coinsurance rate from January 1, 2025 – March 31, 2025, since drug companies raised prices for each of these 64 drugs faster than the rate of inflation. Over 853,000 people with Medicare use these drugs annually to treat conditions such as cancer, osteoporosis, and substance use disorder. Since April 1, 2023, people with Medicare have seen savings on over 120 drugs thanks to Inflation Reduction Act’s Medicare Prescription Drug Inflation Rebate Program.
The Centers for Medicare & Medicaid Services (CMS) is committed to a robust Marketplace Open Enrollment process for consumers so they can easily purchase high-quality, affordable health care coverage. CMS reports that a record 16.6 million consumers signed up for plan year 2025 and will receive up to a full year of coverage beginning January 1. Of those consumers, 2 million are new to the Marketplace this year. This represents selections in the 31 states that use HealthCare.gov. Plan selection continues in most State-based Marketplaces, as well. The next national snapshot will be available in early January.
The footnote at the bottom confirms: "These metrics reflect available Federally-facilitated Marketplaces (FFMs) data through December 18, 2024."
Over 150k Minnesotans have signed up for health insurance since November 1
ST. PAUL, Minn.—Following last year’s incredible enrollment success, MNsure is pleased to report yet another new record for health insurance sign-ups in Minnesota.
Between November 1 and the first deadline (December 18), 151,098 Minnesotans used MNsure.org to sign up for qualified health plans. This represents a 14% increase in private health plan sign-ups compared to the same time last year.
This is excellent news, however, as happens every year with MNsure, it comes with a big caveat.
Idaho actually already launched their 2025 Open Enrollment Period on October 15th, and it only runs through December 16th.*
...*Idaho has continued to doing this even though Nov. 1st has almost always been the official start date and the Biden Admin extended the end date out to Jan. 15th several years ago. The Centers for Medicare & Medicaid Services (CMS) issued new rules last year which I had thought were supposed to crack down on this & bring Idaho in line with other states, but apparently the Gem State was grandfathered in.
Nevada Health Link hasn't published a formal press release about this yet (I'm assuming they're waiting until they actually break 100K to do so, which would be perfect timing since the deadline to enroll for January 1st coverage is New Year's Eve), but I just found this in their December Executive Director's Report from 2 days ago:
OPEN ENROLLMENT 2025
Following the close of week seven, the Plan Year 2025 OEP is the Exchange’s highest performing to date. The annual passive renewals (or Auto-renewals) job was completed in mid-October with a greater than 99.9% renewal success rate.
Holy crap. That's astonishing.
When OEP began on November 1, 91,555 individuals were enrolled in 2025 health coverage, and 16,820 individuals were enrolled in dental coverage, our highest starting numbers ever.
(I'm assuming that's a typo & should be 2024 health coverage, since obviously you can't have anyone enrolled in 2025 coverage prior to OEP launching).