I admit to not really understanding why the Vice story is making the rounds this week in particular. The article is from mid-November, and the study by researchers at the National Bureau of Economic Research which it references was first published in early October...in fact I wrote about it at the time.
Every 10 days, more that 8,000 unvaccinated Republican voters are dying of COVID-19, five times the rate for Democrats, who have had at least 2 vaccination shots.
Eligible MNsure enrollees will save an average of $6,220 this year
ST. PAUL, Minn.—During MNsure’s recent open enrollment period, 129,537 Minnesotans signed up for comprehensive health coverage for 2023. MNsure’s tenth open enrollment period ran from November 1, 2022, through January 15, 2023, and was one of the most successful to date for the state’s health insurance marketplace.
“This year nearly 130,000 Minnesotans will have important financial protections and the peace of mind that comes with being enrolled in comprehensive health coverage available through MNsure,” said MNsure CEO Nate Clark. “MNsure’s tenth open enrollment period was a great success for the organization and the Minnesotans we serve. We helped nearly 60% of enrollees access financial help that will lower their health care costs by an average $6,220.”
Residents Urged to Sign up for Health Coverage as Get Covered New Jersey Open Enrollment Deadline Nears
Total signups over 321K as residents continue to benefit from record savings; Two weeks left to enroll
TRENTON – New Jersey Department of Banking and Insurance Commissioner Marlene Caride today announced that more than 321,000 New Jersey residents signed up for a 2023 health insurance plan through the state’s official health insurance marketplace, Get Covered New Jersey, in the first nine weeks of the Open Enrollment Period that started on November 1, 2022.
With just two weeks left in the Open Enrollment Period, Commissioner Caride urged residents in need of health coverage to review their options and sign up today. Open Enrollment for 2023 health insurance ends January 31st, 2023 in New Jersey.
Washingtonians who qualify for Cascade Care Savings can still sign up and save
The wait is over — Cascade Care Savings is here! Open enrollment may have ended but that doesn’t mean you’re out of luck if you haven’t purchased a plan. A new special enrollment period is available to individuals and families who make up to 250% of the federal poverty level.
“Cascade Care Savings has opened the door for thousands of Washingtonians to secure high-quality health insurance at any time of the year,” Washington Health Benefit Exchange (Exchange) interim CEO Jim Crawford said. “This special enrollment period is available monthly to those who qualify for Cascade Care Savings who are not already in an eligible plan.”
Completed applications/ redeterminations processed through the integrated eligibility system: 25,972
The 108,110 figure may change slightly when the official Open Enrollment Period (OEP) report is released due to last-minute data corrections, but assuming this is the final figure, it means Connecticut's OEP Qualified Health Plan (QHP) enrollment is down just over 4% year over year, from 112,633 during the 2022 OEP. As I noted last week, this is part of a strange trend for 2023: While Medicaid expansion states on the federal exchange are up ~10% vs. last year, most state-based marketplaces (SBMs), including Connecticut, are down somewhat this year.
I'll be posting a second entry addressing that article, the study it cites, and some misinformation about the red/blue divide later this week, but first, let's take a look at where things stand as of mid-January.
Administration policies helped increase coverage among younger adults, Latino individuals, American Indian/Alaska Native, and non-English speaking adults
Today, the U.S. Department of Health and Human Services (HHS) issued a new report showing that Biden-Harris Administration efforts were linked to large gains in health insurance coverage of Americans between 2019 and 2021. The Biden-Harris Administration has made expanding access to health insurance and lowering health care costs for America’s families a top priority, and under its leadership, the national uninsured rate reached an all-time low early in 2022. The report, from the HHS Office of the Assistant Secretary for Planning and Evaluation (ASPE), shows that larger gains in coverage occurred for demographic groups with higher historical uninsured rates, including younger adults, Latino individuals, American Indian/Alaska Native, and non-English speaking adults.
The Maine Department of Health and Human Services (DHHS) is urging Maine residents who lack affordable health insurance to sign up by the deadline of Sunday, January 15, for a 2023 health plan through CoverME.gov, Maine’s health insurance marketplace.
At CoverME.gov, Maine people can compare private plans, apply for financial assistance, and enroll in a 2023 health plan. Health plans offered on CoverME.gov provide quality, comprehensive insurance that protects consumers if they have an accident or major illness and fully pays for preventive screenings for diseases such as cancer and diabetes. This year, more Maine people than ever can get financial help to afford their plans.
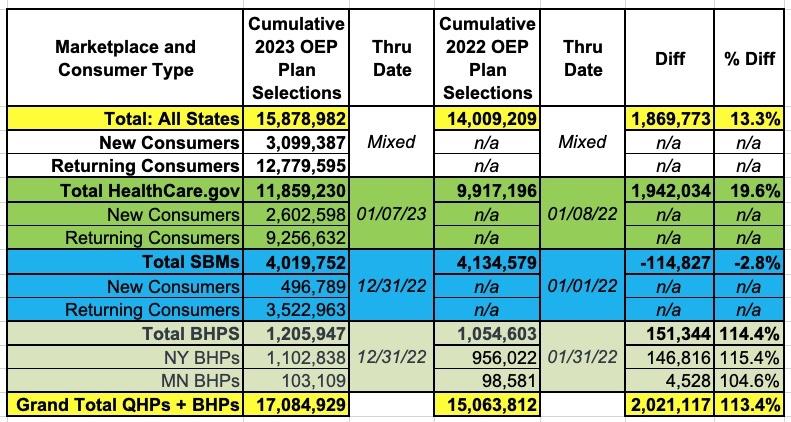
As I noted in yesterday's analysis of the semi-final 2023 Open Enrollment Period report released by the Centers for Medicare & Medicaid Services, one of the most striking data points we're seeing this year is a significant drop in year over year on-exchange enrollment across a number of states operating their own ACA exchanges...even as enrollment continues to surge across states hosted on the federal exchange (HealthCare.Gov).
Overall, QHP enrollment in HC.gov states (Federally Facilitated Marketplaces, or FFMs) is up 19.6% vs. the same point last year, while QHP enrollment in state-based marketplace states (SBMs) is down 2.8% year over year: