Just yesterday I posted the Washington Healthplanfinder's latest monthly report, which showed either 177,613, 170,267 or 167,827 people currently enrolled in exchange QHPs statewide, depending on whether you go by the number who have "selected plans", the number that the carriers have reported as being paid up or the number who the exchange has recorded as having paid.
The first number has been pretty confusing to me over the past few months, because the actual number of people who selected QHPs during the 2016 open enrollment period was reported as just over 200,000 by both the exchange itself as well as in the official national ASPE report, so I wasn't quite sure whether to report the net effectuated enrollment drop since then as being almost none at all or around 15%. I finally went with the 15% figure because dividing into the 177K number just didn't make sense by any other measure.
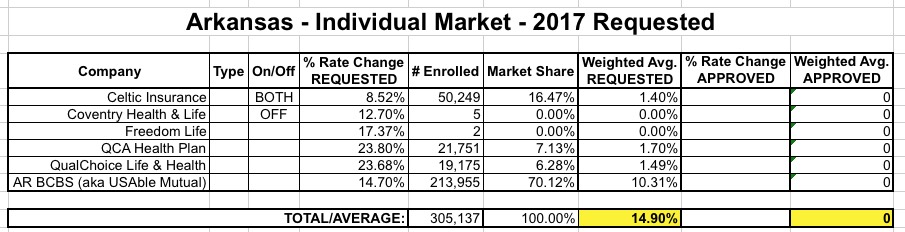
So just last Friday I posted the weighted average requested rate hikes for the Arkansas individual market; it came in at 14.9% overall, which is actually one of the lower statewide averages this year. As a reminder, here's what how the breakout looks:
OK, so 3 major carriers asking to jack up rates 15-24%, plus one at 8.5% and two others with just 7 enrollees between them (one of which is, once again, Freedom Life Insurance). So what?
As regular readers know, I'm currently in the thick of my state-by-state analysis of the requested, weighted average rate changes for 2017 by insurance carriers for the entire ACA-compliant individual market. As of this writing, the overall average looks like it's just a hair over 20% across 28 states + DC.
Does the first sentence above include a lot of clarifiers? Yes, yes it does...and with good reason. I try to be very specific when I discuss this stuff, because it's very easy to get confused about what a given number is actually referring to.
For instance, a few days ago, Avalere Health released their own analysis which concludes that the average requested/proposed premium rates are around 12%. If I left it at that, you might think that either my average is 8 percentage points too high...or that Avalere's is 8 points too low.
Thanks to commenter "Junaed S" who directed me towards this simple, cut 'n dry PDF from the Connecticut Dept. of Insurance detailing the requested rate hikes for the CT individual and small group markets for 2017:
In addition, Anthem has decided not to offer its PPO (Preferred Provider Organization) individual plans in 2017. In all, the Colorado Division of Insurance said Monday around 92,000 people with individual plans from Anthem, UnitedHealth, Humana, and Rocky Mountain Health Plans will have to find other coverage during open enrollment in the fall.
Last month I noted that the Washington Healthplanfinder was reportingcurrently effectuated QHP enrollment at 170,527 as of the end of March, a 15.0% drop from the official number of QHP selections during the 2016 Open Enrollment Period. I also noted that due to some confusion about how the numbers are reported by the exchange, it could also be argued that WA has seen just a 6.6% net drop, depending on how you look at it.
However, since 200,691 is the official number included in the ASPE report, I'm finally letting that one go...and actually, that's OK, because a 15% drop by 3/31 is fairly close to what I would expect anyway (a bit higher than the 13% national drop from last year, but not out of line).
Anyway, the WA exchange just released their May report (with data through the end of April), and it's actually pretty good--there's only been a very slight net drop since March, for an overall drop of just 15.2% from the 200K figure:
A simmering dispute over the risk corridor program has broken into the presidential campaign, with Senator Rubio crowing that an arcane budget move has “kill[ed] Obamacare” and “saved the American taxpayer $2.5 billion.” On account of that move, health plans are set to receive only pennies on the dollar from the risk corridor program, which was supposed to cushion them from big losses.
...The administration has vaguely said that it will “use other sources of funding for the risk corridors payments, subject to the availability of appropriations.” But the budget bill limits the administration’s power to dip into other funds, and a Republican-controlled Congress isn’t likely to appropriate money for a program that’s been decried as an insurer bailout.
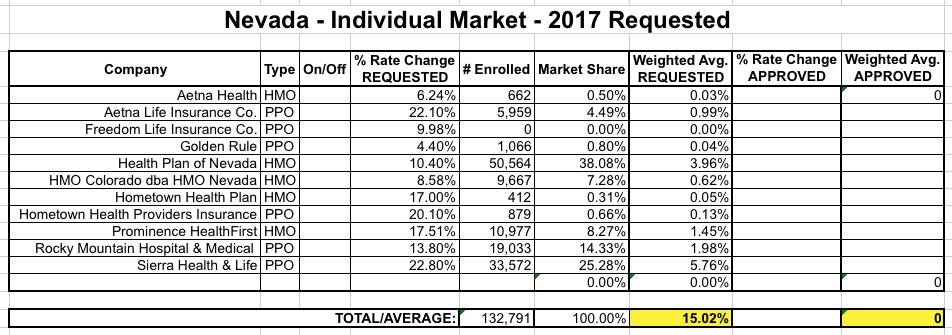
Can I first say that I absolutely love the way Nevada's rate filing database is set up, especially their (apparently proprietary and mandatory) filing format system?
Unlike the standard SERFF database, which is comprehensive but also can be confusing as hell, Nevada's system is simple, clean, easy to navigate and, most of all, every single carrier filing listed displays the number of current enrollees clearly.This is a huge pet peeve of mine, which is understandable given what I'm trying to do here!
OK, that said, here's what things look like in the Silver State:
Delaware is a small state, and only has a total of 4 carriers offering individual polcies (2 on exchange, 2 off). One of those, however, is once again "Freedom Life" which, once again, is asking for precisely a 17.37% rate hike on their almost-certain-to-be-nonexistent enrollees. So...never mind them. That leaves Aetna (split into HMOs and PPOs) and Highmark BCBS offering policies on the exchange, and Golden Rule off the exchange.
Unfortunately, I can't find Golden Rule's actual current enrollment number, but as you can see below, it really doesn't matter:
As you can see, no matter how many enrollees Golden Rule has, their 30.3% average hike request is very close to the 30.6% average of the other carriers. The very most it could do is nudge the weighted average down by a tenth of a point or two, so let's call it 30.5%.