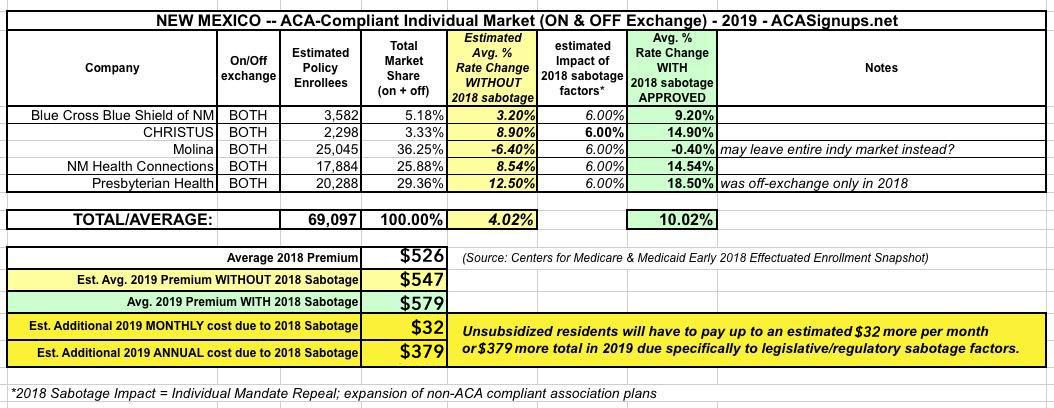
New Mexico was one of the earlier states to post their initial, requested 2019 ACA individual market premium hikes back in June. At the time, the five carriers asked for rate increases ranging from a slight drop (-0.4% for Molina) to as high as an 18.5% increase for Presbyterian Health, which is currently only offering off-exchange policies this year. Based on their preliminary filings, New Mexico was looking at a weighted average increase of around 10.0% next year, which would have been more like 4% if not for this years sabotage efforts by Trump and the GOP (mandate repeal & expansion of #ShortAssPlans):
A few weeks ago, I posted about New Jersey's preliminary 2019 ACA-compliant individual market rate filings. At the time, the official New Jersey Dept. of Banking & Insurance specifically stated that:
AP Exclusive: Modest premium hikes as 'Obamacare' stabilizes
Millions of people covered under the Affordable Care Act will see only modest premium increases next year, and some will get price cuts. That's the conclusion from an exclusive analysis of the besieged but resilient program, which still sparks deep divisions heading into this year's midterm elections.
The Associated Press and the consulting firm Avalere Health crunched available state data and found that "Obamacare's" health insurance marketplaces seem to be stabilizing after two years of sharp premium hikes. And the exodus of insurers from the program has halted, even reversed somewhat, with more consumer choices for 2019.
Normally at this point in the year I only do full rate hike write-ups for states when their approved rate changes are made public by insurance regulators. I'm making an exception for Texas, however, because my preliminary analysis of the statewide average premium changes back in June was missing a huge portion of the market--I only had around half the ACA individual market accounted for, and I repeatedly warned that the missing enrollment and rate change data could easily skew the statewide average higher or lower.
Well, it's early September now, and not only do I have access to pretty much all of the missing data now, some of the rate filings have changed significantly as well. At the time, I estimated Texas carriers as requesting average rate increases of just 1.5% overall, with them dropping around 10.6% if not for the ACA's individual mandate being repealed and Trump's expansion of #ShortAssPlans.
I received a tip about this early this morning...which, unfortunately, I was unable to scoop anyone with due to being bogged down/caught up with the #TexasFoldEm drama.
Montana insurer wins lawsuit against feds over unpaid cost-sharing reduction payments
Several health insurers have sued the U.S. government over its failure to make cost-sharing reduction payments that help lower healthcare costs for certain consumers. One just scored the first victory. The U.S. Court of Federal Claims ruled in favor of Montana Health Co-op, which sued the federal government for $5.3 million in unpaid cost-sharing reduction payments, finding that the government violated its obligation under the Affordable Care Act when it stopped paying the CSRs in October 2017."
The rest of the article is behind a paywall, but the gist of it is as follows:
U.S. District Court Judge Reed O'Connor, a George W. Bush appointee, vigorously questioned attorneys during the three-hour hearing but gave no indication when he would rule.
Lawyers for the Trump administration partially agreed with the red states' argument, concluding that the removal of Obamacare's individual mandate requires striking down the law's insurance provisions, including protections for people with preexisting medical conditions.
But the administration disagreed on the need for immediate action, arguing that any remedies should not be applied until next year.
In June 2018, President Trump’s administration announced – as part of a lawsuit known as Texas v. United States, brought by 20 Republican state attorneys general – it will no longer defend the ACA’s protections for people with pre-existing medical conditions.