Insurance Commissioner approves rates insurers filed for 2018; Cost to cover CSRs has been added to silver plan premiums
On September 20, the Tennessee Department of Insurance and Commerce (TDIC) announced that the state had approved the rates that insurers had filed for 2018. However, the announcement indicated that Cigna’s approved average rate increase was 42.1 percent, which was based on the filing Cigna submitted in June 2017. An updated filing, with an average rate increase of 36.5 percent, was submitted in August, and TDIC confirmed by phone on September 21 that the updated filing was approved. The slightly smaller rate increase is due to Cigna’s decision to terminate some existing plans and replace them with new plans).
The following average rate increases were approved for 2018 individual market coverage:
New Mexico Health Connections, the nonprofit co-op insurance company formed under the Affordable Care Act, is selling its small group and commercial business to a for-profit company under a restructuring plan that will create a new insurance company that will be able to go after business the struggling nonprofit couldn’t.
...The Washington, D.C.-based Evolent will acquire NMHC’s 22,000 commercial members. NMHC will continue to exist with a few employees and presumably continue to sell individual policies on the New Mexico Health Insurance Exchange. NMHC has 10,000 individual members through the insurance exchange.
...Hickey told ABQ Free Press that the deal will allow the new firm to go after business that NMHC couldn’t, things like Medicare Advantage, federal employees and, eventually, Medicaid. It also gives the new firm capital reserves that NMHC didn’t have, he added.
In August I wrote that the situation in North Dakota was pretty straightforward: Three carriers on the individual exchange (BCBS, Medica and Sanford), requesting average rate hikes of around 24%, 19% and 12% respectively for an average increase of 23% assuming CSR payments are made, or a bit higher (28%) if they aren't.
Yesterday, however, with the final contract signing deadline having passed on the 27th, Louise Norris reports that one of the three carriers, Medica, was forced to drop out of the market at the last moment...not because they wanted to, but because the ND insurance dept. insisted on carriers pricing 2018 premiums on the assumption CSRs will be paid for the full year.
Medica understandably refused to take that risk (the odds of CSRs being guaranteed are virtually nil, and the odds of them being paid each and every month, as they're supposed to, is only so-so), so they dropped out instead.
Back in August, I reported that thanks to their just-approved federal reinsurance program, Alaska (which has only a single individual market carrier with the most expensive premiums in the country) is looking at an impressive 22% average decrease in their indy market premiums next year. However, that was based on the assumption that CSR reimbursement payments would not be made (or at least not guaranteed).
Alaskans buying health insurance on the individual market will see a decrease of 26.5 percent in rates next year, the sole insurer in the state announced Tuesday.
Alaskans had been paying some of the highest premiums in the nation.
The White House approved the use of military aircraft for multi-national trips by Health and Human Services Secretary Tom Price to Africa and Europe this spring, and to Asia in the summer, at a cost of more than $500,000 to taxpayers.
The overseas trips bring the total cost to taxpayers of Price’s travels to more than $1 million since May, according to a POLITICO review.
CMS Announces Special Enrollment Periods for Americans Impacted by Recent Hurricanes Agency provides special open enrollment periods for 2017 Medicare and Exchange coverage
As a result of Hurricanes Harvey, Irma, and Maria, the Centers for Medicare & Medicaid Services (CMS) will make available special enrollment periods for all Medicare beneficiaries and certain individuals seeking health plans offered through the Federal Health Insurance Exchange. This important step gives these individuals and families who have been impacted by the hurricanes the opportunity to change their Medicare health and prescription drug plans and gain access to health coverage on the Exchange immediately if eligible for a special enrollment period.
More to the point, however: What other significance does not including CSR funding have?
Well, first of all, is it possible that they'll slip CSRs in before the vote? I suppose so, but consider this:
The final deadline for the insurance carriers to actually sign their contracts for 2018 is Sept. 27th, just 8 days from now.
The end of the 2017 fiscal year (i.e., the deadline for the GOP to try and cram through Graham-Cassidy with only 50 Senate votes) is Sept. 30th.
The CBO is "aiming" to provide a "preliminary assessment" of Graham-Cassidy "early next week" which I presume means Monday the 25th or Tuesday the 26th.
I assume the other steps (parlimentary ruling, vote-a-rama, etc) would take place on Wednesday the 27th, the same day the contracts have to be signed.
Yom Kippur is the evening of the 29th, running through Saturday the 30th. I can't imagine even McConnell would be that much of a dick to schedule the vote then.
That leaves Thursday the 28th or Friday the 29th for the actual vote itself.
That's a day or two after the carrier contracts have been signed.
Then, just this week, after Senators Collins, McCain, Paul—and potentially Murkowski—announced their opposition to the bill, the GOP leadership announced that the Senate would not vote on Graham-Cassidy. Given budget reconciliation rules, the Senate only has until September 30th to pass a repeal bill with just 50 votes (Vice President Pence then casting the tie-breaking vote). Thus, it would appear that repeal efforts will be delayed until the spring of 2018 when fiscal year 2019 begins, and new budget reconciliation rules are established. All of that said, I am sick and tired of sitting on pins and needles as this process has unfolded. Based on the submissions I received this week, many of my colleagues seem to share my sentiments, as very few posts focused on Graham-Cassidy. In recognition of that, I present you with the “Repeal Fatigue” edition of the Health Wonk Review.
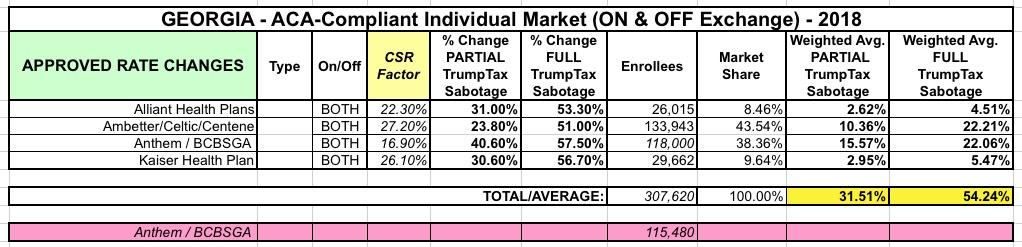
INSURANCE DEPARTMENT RELEASES PROPOSED RATES FOR 2018 HEALTHCARE EXCHANGE
Atlanta – Insurance Commissioner Ralph Hudgens announced today that his office had submitted proposed 2018 health insurance rates to the Centers for Medicare and Medicaid Services (CMS) for the federally-facilitated Healthcare Exchange for final federal approval.
“Today my office submitted 2018 Obamacare rates to Washington D.C. for approval,” Hudgens said. “In its fifth year, Obamacare has become even more unaffordable for Georgia’s middle class with potential premium increases up to 57.5 percent. I am disappointed by reports that the latest Obamacare repeal has stalled once again and urge Congress to take action to end this failed health insurance experiment.”
Trump administration abruptly drops out of Obamacare events in Mississippi
“It’s clearly sabotage.”
For the past three years, the US Health and Human Services Department has partnered with a health advocacy group in Mississippi on an education tour before Obamacare enrollment started. They would meet around the states with groups that sign people up for coverage — state officials, health centers, insurance brokers, and the like — to prepare for open enrollment.
Up until Monday, Roy Mitchell, executive director of the Mississippi Health Advocacy Program, thought these events were going forward in the coming weeks as planned. He had even asked HHS just last week for biographies of the officials they’d be sending.



{kind=link}