After some last-minute drama in one state and a surprising lack of drama in another, both New Jersey and Pennsylvania have officially passed bills allowing them to each establish their own ACA exchanges and enrollment platforms, splitting off from the federal exchange and HealthCare.Gov:
UPDATE 8/20/19: I originally posted this in late June. Since then, there have been several important developments: Joe Biden and Kamala Harris have formally rolled out their own official healthcare overhaul plans, with Harris splitting off from Bernie Sanders' fully-mandatory "Medicare for All" bill to her own variant, which keeps the name but has similarities to "Medicare for America". Also, Eric Swalwell and John Hickenlooper have dropped out (ok, not every development was major).
I've updated the post to reflect these changes, while also updating the table graphic, which I've also simplified by removing Swalwell, Hickenlooper and most of the other bottom-rung candidates. I'm keeping everyone who's qualified for the September/October debates as of this writing, plus Tulsi Gabbard, Jay Inslee and Tom Steyer, each of whom is partly qualified.
Not much of an entry, but still: A month ago, the Oregon Division of Financial Regulation posted the requested 2020 rate changes for the Individual and Small Group health insurance markets: 3.3% on average for the Indy market, 8.7% for the sm. group market.
Today, after reviewing the requests from the insurance carriers, the department has posted their "semi-final" rates. These may still see some additional tweaking before the final, approved rates are locked in, but the odds are that these will be the final rates:
Salem — Oregonians can now see the state’s preliminary rate decisions for 2020 individual and small employer health insurance plans. The Division of Financial Regulation must review and approve any rates before they can be charged to policyholders.
Preliminary rate decisions are for individuals who buy their own coverage rather than getting it through an employer and for small businesses.
HOLT: Senator Warren, you signed on to Bernie Sanders’ Medicare-for-all plan. It would put essentially everybody on Medicare and then eliminate private plans that offer similar coverage. Is that the plan or path that you would pursue as president?
WARREN: So, yes. I'm with Bernie on Medicare for all. And let me tell you why.
I spent a big chunk of my life studying why families go broke. And one of the number-one reasons is the cost of health care, medical bills. And that's not just for people who don't have insurance. It's for people who have insurance.
Senator Warren, thank you so much for being here this evening and your tireless advocacy for universal health care. As a supporter of universal health care and an advocate for organized labor, I do worry about the current bill...that would eliminate the private health employer-based plans that so many unions have advocated for. Can you explain how Medicare for all would be better for workers than simply improving the Affordable Care Act?
WARREN: OK, so it's a good question. Let's start with our statement that we should make every time we start to talk about changes in our health care, and that is health care is a basic human right and we fight for basic human rights. And then let's put these in order, because I appreciate that your question starts with the Affordable Care Act. Let's all remember when we're talking about what's possible, let's start where we are and the difference between Democrats and Republicans.
New Jersey’s most powerful state lawmaker said he will delay a vote to create the state’s own online shopping portal for health insurance, one of Gov. Phil Murphy’s priorities intended to guard against the possible repeal of the Affordable Care Act.
The delay means the state won’t meet an Aug. 1 deadline to submit an application to the federal government to create the exchange. The anticipated launch of a Fall 2020 open enrollment period would have to be postponed until 2021, a group of health policy experts warned.
State Senate President Stephen Sweeney, D-Gloucester issued a statement Tuesday affirming his support for creating New Jersey’s own health exchange. Sweeney said he just disagrees with the way fellow lawmakers want to go about it because it doesn’t include a means to automatically enroll low-income people into the Medicaid program.
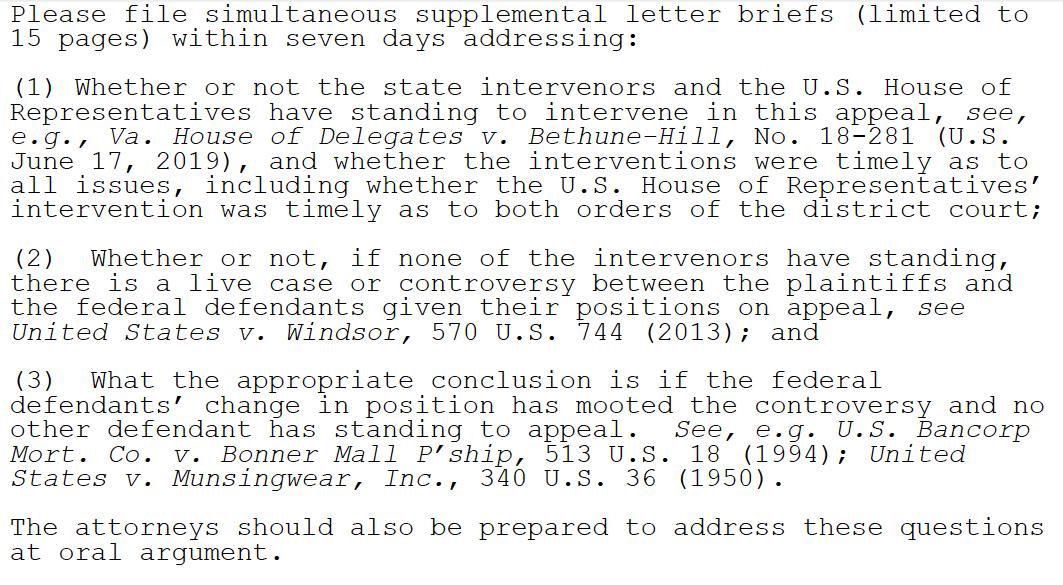
Jibbers Crabst on a stick. Any time University of Michigan Law Professor Nicholas Bagley begins his Twitter threads with a screenshot of legalese, it's bad news.
First, here's his full thread:
The panel in the Fifth Circuit that's about to hear Texas v. United States has just asked for further briefing on standing -- and in particular on whether the intervenor states and the House of Representatives can properly appeal the case.
I know I rip on Republicans a lot here at ACASignups.net, and I stand by pretty much all of it. Once in a while, however, a GOP member of Congress does do (or tries to do) something useful when it comes to healthcare policy...and the name most often attached to that is Senator Lamar Alexander of Tennessee. Alexander happens to be retiring, I should note. These two facts may or may not be connected, but I digress.
In any event, Sen. Alexander and Democratic Senator Patty Murray of Washington State have been working together for quite some time now on several healthcare bills to help stabilize the ACA, reduce drug prices and so forth, to varying degrees of success. I may not have agreed with most of Alexander's ideas, but he seems to be genuinely interested in improving the situation...and of course I can't say enough good things about Sen. Murray.
Regular readers may have noticed that I didn't post a single blog entry on Tuesday even though there's been a ton of healthcare policy stuff going on. No, I didn't take the day off; I started poring over a spreadsheet at around 10am and was working on it almost nonstop all day.
Big news: SCOTUS is taking up the ACA risk corridors case. GOP's decision to stymie that program arguably did the most damage to the ACA marketplaces. https://t.co/VeMRcd5MYn
When the ACA was first developed and voted on, lawmakers knew that the disruption to the individual health insurance market was going to be pretty rocky for the first few years, so they put three types of market stabilization programs into place. They were known as the "Three 'R's"...Risk Adjustment, Reinsurance and Risk Corridors:
...Risk adjustment interrupts these cycles by doing exactly what its name implies. It adjusts for differences in the health of plans’ enrollees by redistributing funds from companies with healthier-than-average customers to plans with sicker-than-average customers. Such transfers could occur within or across health plan tiers in the exchanges (bronze, silver, gold, platinum). All the redistributed monies come from insurance companies in the marketplaces. No taxpayer bailout here.