Yes, I'm back from Netroots Nation 2019, and yes, I know that Joe Biden just rolled out his official healthcare policy proposal for the 2020 Presidential election.
I still have to read his plan through and will write up my thoughts about it later today, but before that, I have to take care of this:
I'm happy to report that our panel did indeed make the final cut, and will be happening this Friday, July 12th:
FIX THE DAMN HEALTHCARE: SORTING OUT ACA 2.0, MFA, MED4AM AND MORE!
Friday, Jul. 12 4:30 PM, Room: 118C
The healthcare landscape is confusing and exciting in 2019. Reining in Big Pharma, strengthening the ACA, adding public options, “Medicare for America” or “Medicare for All”… the alphabet soup of plans can be confusing. Can improvements be implemented before 2021 at the federal level or is it all up to the states? And what about the latest lawsuit looming over everything? We’ll go beyond the slogans and into the details: How are the proposals similar and different, and what do patients, caregivers and other invested parties think.
UPDATE 8/20/19: I originally posted this in late June. Since then, there have been several important developments: Joe Biden and Kamala Harris have formally rolled out their own official healthcare overhaul plans, with Harris splitting off from Bernie Sanders' fully-mandatory "Medicare for All" bill to her own variant, which keeps the name but has similarities to "Medicare for America". Also, Eric Swalwell and John Hickenlooper have dropped out (ok, not every development was major).
I've updated the post to reflect these changes, while also updating the table graphic, which I've also simplified by removing Swalwell, Hickenlooper and most of the other bottom-rung candidates. I'm keeping everyone who's qualified for the September/October debates as of this writing, plus Tulsi Gabbard, Jay Inslee and Tom Steyer, each of whom is partly qualified.
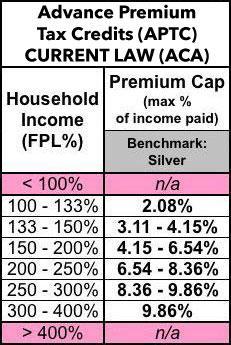
As I've noted several times, one of the biggest flaws in the Affordable Care Act is a very simple one on paper: The Subsidy Cliff. People who enroll in ACA exchange policies are entitled to financial assistance on a sliding scale...but only if their household incomes fall between 100-400% of the Federal Povery Level. Those below the lower threshold (actually, below 138% FPL) are expected to enroll in Medicaid, but those over the upper threshold of 400% FPL (around $50,000/year for a single person, roughly $103,000/year for a family of four) are completely on their own.
Here's the current federal premium subsidy formula (the precise premium cap percentages change slightly from year to year...and the Trump Administration is even messing with that a bit, so I'm not sure what it'll be in 2020):
As a reminder, here's the eight bills which passed the full House:
H.R. 938, the "Bringing Low-cost Options and Competition while Keeping Incentives for New Generics (BLOCKING) Act of 2019," introduced by Reps. Kurt Schrader (D-OR) and Buddy Carter (R-GA), would discourage parking of 180-day exclusivity by a first generic applicant that is blocking the approval of other generics.
H.R. 1499, the "Protecting Consumer Access to Generic Drugs Act of 2019," introduced by Rep. Bobby Rush (D-IL), would make it illegal for brand-name and generic drug manufacturers to enter into agreements in which the brand-name drug manufacturer pays the generic manufacturer to keep a generic equivalent off the market.
Last May, I noted that Vermont was supposedly joining Massachusetts, New Jersey (and later in the year, the District of Columbia) in reinstating the ACA's Individual Mandate Penalty, which added an additional tax to people who don't enroll in ACA-compliant healthcare coverage (whether private or public) and who don't qualify for an exemption due to an affordability threshold, hardship or some other qualifying reason.
Strike One:Vermont's mandate won't go into effect until 2020, leaving a one-year gap. This bill getting signed is still good news, but mostly irrelevant for 2019. The "coordinated outreach efforts" part is really more of a counter to the Trump Administration's slashing of the ACA's marketing/outreach budget...but not really, since Vermont already runs their own exchange and should have their own marketing/outreach budget anyway. So this is more of a token gesture, I'd guess.
Legislation calls for reinsurance program to aid people with extremely high health insurance premiums
Lawmakers have introduced legislation this week that would create a reinsurance program to help lower the cost of premiums for Delawareans who do not get insurance through their employers.
House Bill 176, which has no Republican co-sponsors, would stabilize the individual health insurance market and help Delawareans struggling with extremely highhealthcare costs to get relief, a release from House Democrats stated.
PROVIDENCE — The state Senate approved legislation Thursday intended to protect Rhode Islanders’ access to health insurance in the face of threats to the federal Affordable Care Act.
The legislation was sponsored by Sen. Joshua Miller, D-Cranston, chairman of the Senate Health and Human Services Committee. The House version of the bill was sponsored by Rep. Joseph M. McNamara, D-Warwick, chairman of the House Health, Education and Welfare Committee. The bill aims to ensure that the standards of the Affordable Care Act remain in effect in Rhode Island, even if the courts or Congress were to eliminate the federal laws that created it.
...voters were only dimly aware of candidates’ and elected officials’ health proposals.
...These voters are not tuned into the details — or even the broad outlines — of the health policy debates going on in Washington and the campaign, even though they say health care will be at least somewhat important to their vote.
Many had never heard the term “Medicare for all”...