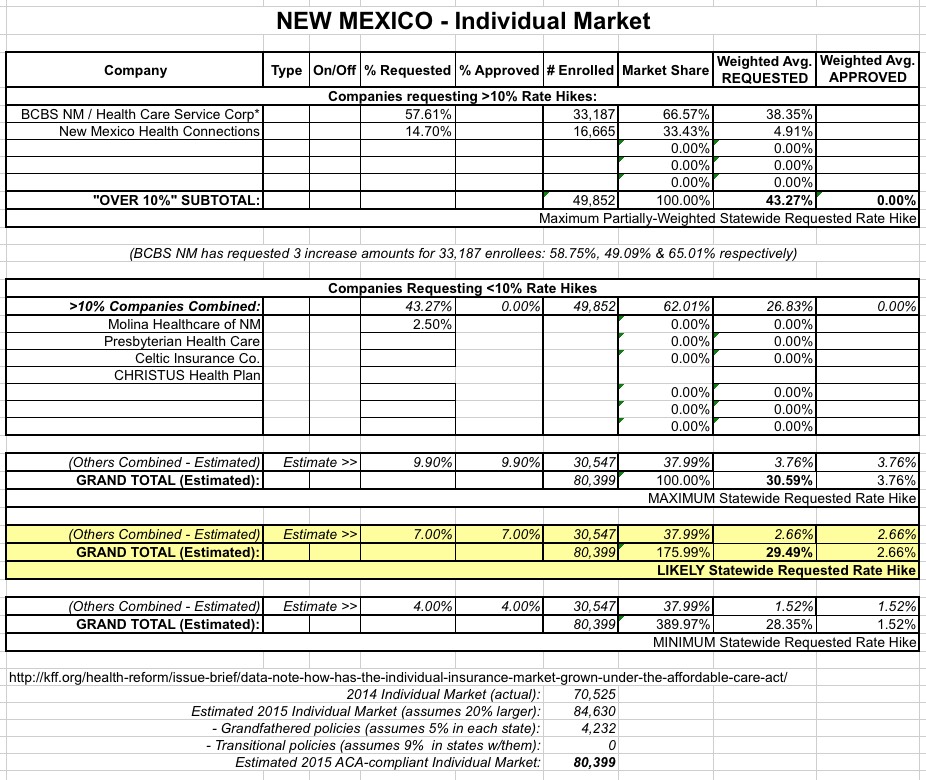
IMPORTANT:See this detailed explanation of how I've come up with the following estimated maximum requested weighted average rate increases for New Mexico.
As explained in the first link above, I've still been able to piece together rough estimates of the maximum possible and most likely requested average rate increase for the New Mexico individual market:
Again, the full explanation is included in the Missouri estimate linked at the top of this entry, but to the best of my knowledge, it looks like the companies with rate increases higher than 10% come in at a weighted 43.3% increase, but only make up about 62% of the total ACA-compliant individual market, with several other companies with approved increases of less than 10% (decreases in some cases) making up the other 38%.
Unfortunately for my purposes, most of the info here relates to dollars (which is understandable for earnings reports, of course), but therewas one relevant enrollment number given:
Molina Healthcare
Molina is reporting $39 million in net income for the latest quarter on $3.5 billion in revenue, compared with $7.8 million in net income on $2.3 billion in revenue for the second quarter of 2014.
The company ended the quarter providing or administering medical coverage for 3.4 million people, up from 2.3 million people a year earlier.
Enrollment in the company's PPACA public exchange qualified health plans (QHPs) increased to 261,000 from 18,000.
That's an impressive year over year increase...over 14x as many ACA exchange enrollees for Molina this year than last.
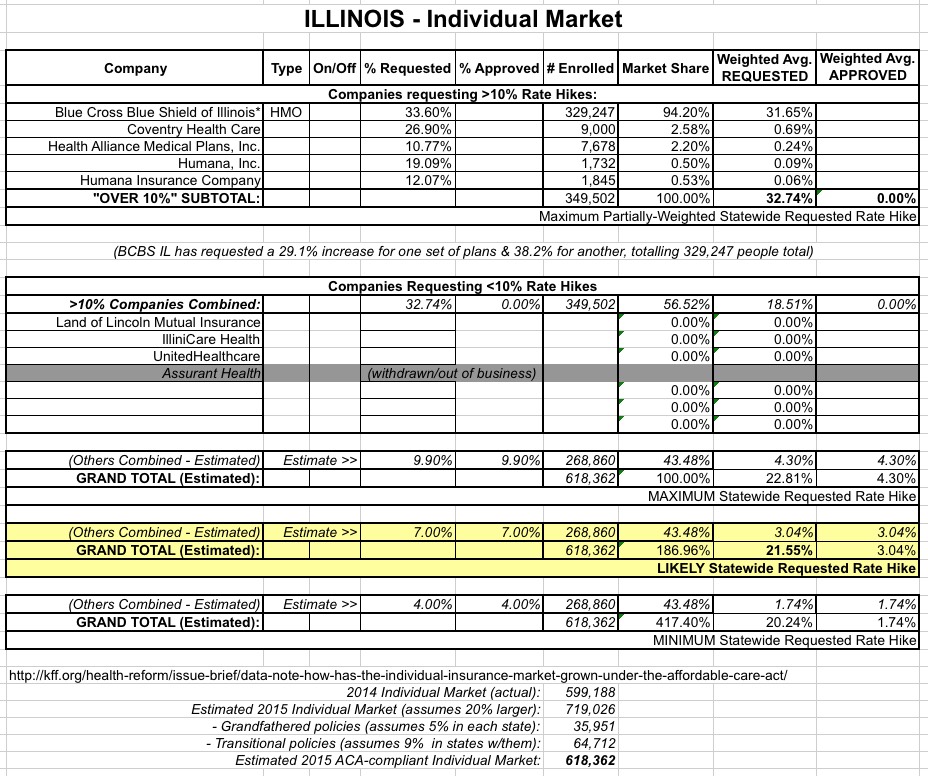
IMPORTANT:See this detailed explanation of how I've come up with the following estimated maximum requested weighted average rate increases for Illinois
As explained in the first link above, I've still been able to piece together rough estimates of the maximum possible and most likely approved average rate increase for the Illinois individual market:
Again, the full explanation is included in the Missouri estimate linked at the top of this entry, but to the best of my knowledge, it looks like the companies with rate increases higher than 10% come in at a weighted 32.7% increase, but only make up about 57% of the total ACA-compliant individual market, with several other companies with approved increases of less than 10% (decreases in some cases) making up the other 43%.
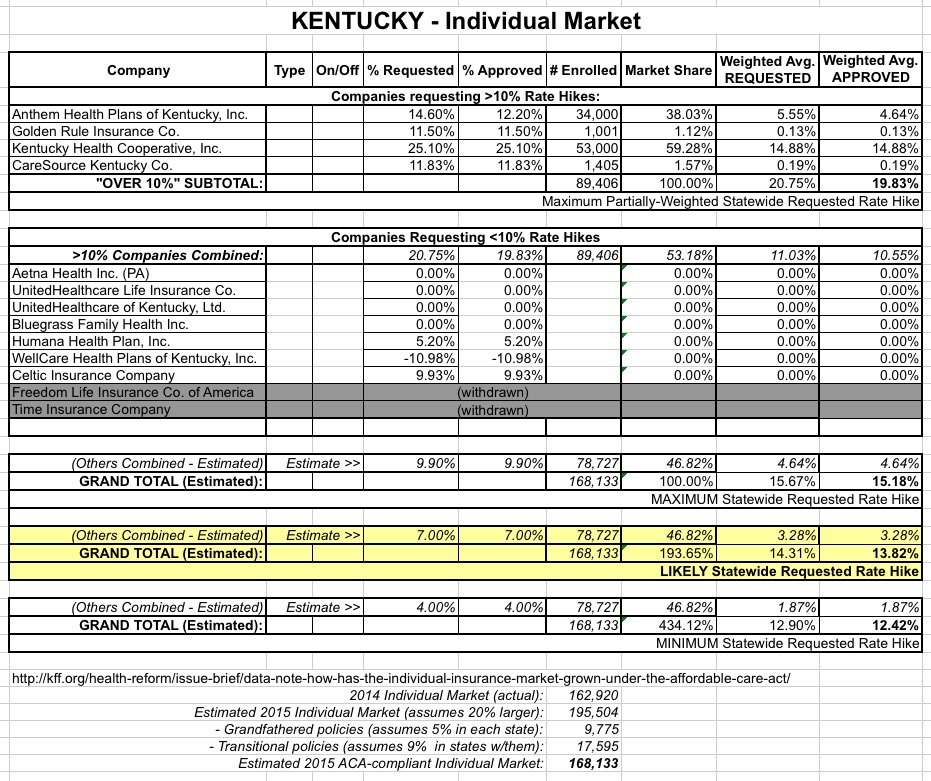
IMPORTANT:See this detailed explanation of how I've come up with the following estimated maximum approved weighted average rate increases for Kentucky.
Fortunately, as I explain in the first link above, I've still been able to piece together rough estimates of the maximum possible and most likely approved average rate increase for the Kentucky individual market:
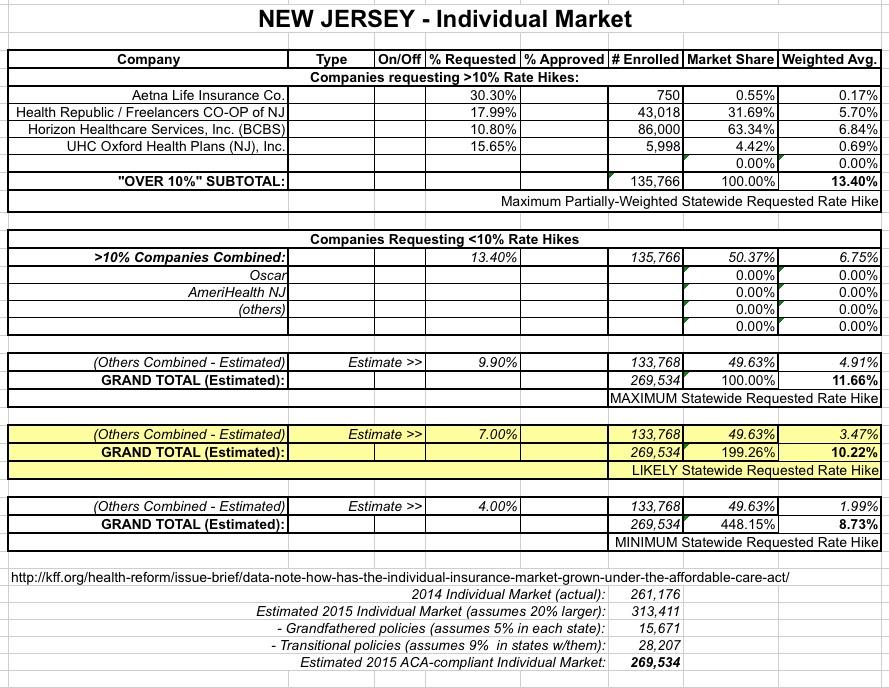
IMPORTANT:See this detailed explanation of how I've come up with the following estimated maximum weighted average rate increase request for New Jersey
Assuming you've read through the explanation linked to above, here's my best estimate of the maximum possible and most likely average rate increase requests for the New Jersey individual market:
Again, the full explanation is included in the Missouri estimate, but to the best of my knowledge, it looks like the companies requesting rate increases higher than 10% come in at a weighted 13.4% increase, but only make up about 50% of the total ACA-compliant individual market, with several other companies (Oscar, AmeriHealth & possibly other off-exchange only companies) requesting increases of less than 10% (or possibly even decreases in some cases) and making up the other half.
Now that the Supreme Court has rendered its decision in King v. Burwell on federal subsidies under the Affordable Care Act (ACA) and Open Enrollment is approaching, there is no better time to reflect on the important mission of access to affordable and quality health coverage for the residents of all states. Health insurance is complex; it engages a range of stakeholders from state agencies and insurance carriers to brokers and solution providers, it requires eligibility determination, various payment models, and a myriad of funding mechanisms, to name a few.
Senate Republican leaders this week narrowly averted an intra-party battle over ObamaCare by again promising to get a repeal bill to the president’s desk through budget reconciliation.
Last week I took the known 2016 Florida rate increase requests (around 14.7% weighted average for 10 companies with around 713,000 enrollees) and took my best shot at trying to estimate what the rest of Florida's ACA-compliant individual market might look like.
In order to do this properly, I'd need 2 pieces of data: First, the weighted average increase request for the 6 additionalcompanies which I didn't already have rate requests for; and second, the total ACA-compliant enrollment number for those 6 companies.
During the fiscal year that ended June 30, 2014, the most recent for which data is available, Planned Parenthood affiliates around the country received $528.4 million in government funds (a combination of state, federal and sometimes local government dollars), according to the organization's ownannual report and information it's required to share with the IRS.
CONGRESSIONAL BUDGET OFFICE
Keith Hall, Director
U.S. Congress
Washington, DC 20515
August 3, 2015
Honorable Mike Enzi
Chairman
Committee on the Budget
United States Senate
Washington, DC 20510
Re: Budgetary Effects of S. 1881
Dear Mr. Chairman:
Last week, CBO provided the following information in response to a request for an estimate of the budgetary effects of S. 1881:
S. 1881, which would prohibit federal funds from being made available to Planned Parenthood Federation of America or any of its affiliates, could affect direct spending for the Medicaid program; however, CBO has not determined whether the legislation would increase or decrease the program’s spending. Completing an estimate of such effects would take some time.
MAYAGÜEZ, P.R. — The first visible sign that the health care system in Puerto Rico was seriously in trouble was when a steady stream of doctors — more than 3,000 in five years — began to leave the island for more lucrative, less stressful jobs on the mainland.
Now, as Puerto Rico faces another hefty cut to a popular Medicareprogram and grapples with an alarming shortage of Medicaid funds, its health care system is headed for an all-out crisis, which could further undermine the island’s gutted economy.
Now that Congress and the courts have failed to overhaul Obamacare, states are eyeing the only current remaining opportunity to modify the healthcare law — this time from the inside out.