Two bits of news out of the DC exchange today: First, they announced that the uninsured rate has been slashed in half over the past 3 years thanks in no small part to the Affordable Care Act. Not a huge shocker given the recent surveys/studies released by the CDC, Gallup, Kaiser and so on of late, but still good to see:
Washington, DC – A new survey by the Center for the Study of Services conducted for the DC Health Benefit Exchange Authority (DCHBX) concludes that the District of Columbia made huge gains during the most recent open enrollment period to provide access to health insurance coverage to people who were previously uninsured. Results from this survey show that more than 25,500 people, who were not previously covered in 2015, gained access to health insurance coverage in 2016 through DC Health Link, the District’s online health insurance marketplace.
UnitedHealth Group Inc., the biggest U.S. health insurer, is scaling back its experiment in Obamacare markets as its Harken Health Insurance Co. startup withdraws from the two exchanges where it was selling plans.
Harken will not offer individual plans through Obamacare exchanges in Georgia and Chicago in 2017, the company said Thursday in an e-mailed statement. It will continue to offer individual plans off the exchange, Harken said.
As commenter ME notes, there are currently around 22,800 Harken enrollees in Illinois and another 10,500 in Georgia. I have no idea what the on/off exchange ratio is, however, so the number of people who will actually have to shop around will be up to 33,300; assuming, say, 2/3 are on the exchange, that would be roughly 22,000 people.
BATON ROUGE — The number of people who have signed up for Louisiana's Medicaid expansion program continues to grow, surpassing 300,000.
The Louisiana Department of Health released the latest figures Monday, saying more than 304,000 people are enrolled for the coverage that began July 1.
The department says nearly 12,000 Medicaid expansion enrollees have received preventive services through the government-finance insurance program so far, like cancer screenings, colonoscopies, and mammograms.
The maximum number of Louisianans eligible for Medicaid expansion in the state is supposedly around 375,000. Enrollment began in June (though the program didn't actually go into effect until July), so that's 81% of the total enrolled within just 3 1/2 months.
A few weeks back, the CDC released the results of the latest National Health Interview Survey, considered the gold standard for measuring U.S. insured/uninsured rates; it concluded, unsurprisingly, that thanks to the ACA, the uninsured rate in the United States has plummeted from 16% in 2010 to it's lowest level in pretty much forever, just 8.6%.
NHIS's methodology is more comprehensive than that of, say, the Gallup-Healthways quarterly surveys, which doesn't include children, so the numbers are understandably a bit different, but the results are unquestionable: For whatever other flaws it may have, the Affordable Care Act has dramatically lowered the uninsured rate in the United States.
Normally I post screenshots from the revised/updated SERFF filings and/or updates at RateReview.HealthCare.Gov, but it takes forever and I think I've more than established my credibility on this sort of thing, so forgive me for not doing so here. Besides, #OE4 is approaching so rapidly now that this entire project will become moot soon enough, as people start actually shopping around and finding out just what their premium changes will be for 2017.
The other reason I'm not too concerned about documenting the latest batch of updates/additional data is because in the end none of it is making much of a difference to the larger national average anyway; no matter how the individual carrier rates jump around in various states, the overall, national weighted average still seems to hover right around the 25% level.
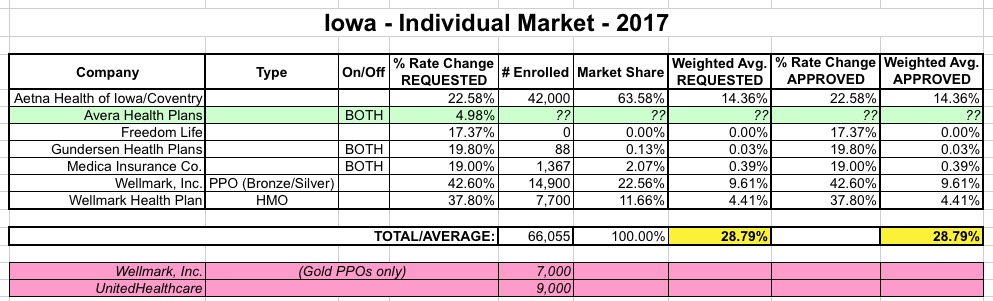
Still, for the record, here's the latest...in four states (Iowa, Indiana, Maine & Tennessee) I've just updated the requested and/or approved average increases. In the other four (Massachusetts, Montana, North & South Dakota) I've added the approved rate hikes as well.
I've written a lot in the past about off-season exchange enrollments, otherwise known as SEPs (Special Enrollment Periods). For the most part, SEPs refer to people who enroll in individual policies after the official Open Enrollment period. They're allowed to do so for a variety of reasons: If they move outside of their rating area; if they get married or divorced; if they give birth or adopt a child; if they get out of prison; if they're discharged from the military; or, in most cases, if they lose whatever current healthcare coverage they have due to losing a job, etc.
Over the past 3 years I've estimated that somewhere between 7,000 - 9,000 people sign up for ACA exchange coverage via SEPs every day during the off season, and I've been proven pretty much dead on target on the rare occasions that hard data has been released. Now, that may have dropped somewhat this year since CMS has cracked down on verifying SEP eligibility, but that's still an uknown. Every time someone selects a QHP via one of the ACA exchanges, the official 12.7 million tally for 2016 continues to go up.
At the same time, there has obviously been a lot of of attrition as people drop their policies throughout the year. The official effectuated enrollee number as of March 31st was down to 11.1 million people...a 13% drop from the 12.7 million who had selected QHPs as of the end of January.
Wellmark Blue Cross and Blue Shield announced Tuesday that it will narrow its choices for individual Affordable Care Act plans in Iowa and will eliminate ACA individual plans in South Dakota altogether in 2017.
First, some clarification: Wellmark isn't on the exchange to begin with, and wasn't planning on joining it in SD next year, so this is a rare case of a carrier dropping their off-exchange individual market offerings. Since all of Wellmark's indy enrollees in South Dakota are paying full price, this one can't be blamed on APTC enrollees being sicker than average, etc.
As for Iowa, it's more of a mixed bag...Wellmark is basically swapping out higher end PPO plans for lower end HMO, which is pretty much the trend everywhere:
Every month I post an entry about the official CMS Medicaid enrollment report, documenting the increase in Medicaid enrollment since ACA expansion went into effect. The numbers were increasing dramatically every month for nearly two years, but started slowing down last fall as most of the expansion states started maxing out on their eligible enrollees.
An important reminder from an anonymous tipster for any Illinois resident who was enrolled in a policy via the now-defunct "Land of Lincoln" Co-Op:
Hey hey. Just wanted to pass some info to you in case you can get it out there. As of last week (not sure the date - either the 15th or the week after) only 34% of LOLH members had taken advantage of the SEP. Spoke with legislators yesterday to get the word out, but since the deadline is Friday, we are trying to get the word out for people to get enrolled.
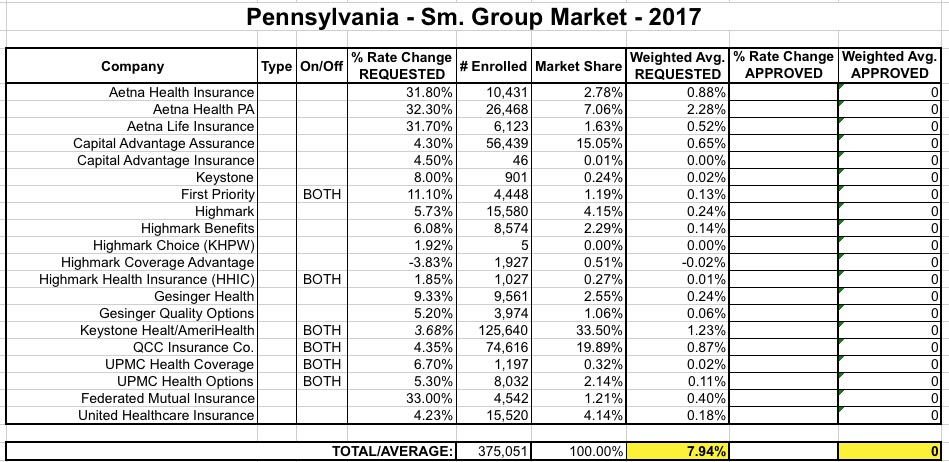
Yesterday I hobbled together the weighted average rate hikes (either requested or approved) for the ACA-compliant small group markets across 15 states. In 4 of these states, I hadn't yet tallied the weighted average, so I temporarily used the median increase for each. In the case of Pennsylvania, the range was from a 3.8% decrease to a 33% increase, with a midpoint of around 14.6%.
Today, however, I've actually plugged in the enrollment numbers for each sm. group carrier in Pennsylvania based on their 2017 rate request filings, and have come up with a weighted average of just 7.9%: