TRENTON — In a bulletin issued today, the New Jersey Department of Banking and Insurance issued guidance to insurance carriers on health insurance coverage for childhood immunizations.
The Department advises that, regardless of federal actions relating to the childhood immunization schedule, it expects carriers to provide coverage for childhood immunizations recommended by the New Jersey Department of Health, including for the hepatitis B vaccination series, in accordance with State law and without cost sharing or the imposition of additional barriers.
12/5/25: Update on Provider Network Information in Plan Comparison Tool
We are aware of several provider network inaccuracies in our Plan Comparison Tool. The inaccuracies are related to Anthem plans.
The network issues related to Anthem plans are limited to Northern Light providers. We expect the Anthem network to be corrected by December 16. In the interim, consumers may use Anthem's Provider Lookup Tool (external to CoverME.gov).
Oy...December 16th? That's the day after the initial Open Enrollment Deadline passes. Sheesh.
For nearly a year now, I've been writing about the upcoming expiration of the enhanced ACA premium tax credits (eAPTC) which have been in place for the past five years. They're currently scheduled to expire at the end of December, less than 2 months from today.
Over the past few weeks as the various ACA exchange websites brought their 2026 ACA window shopping live, I've started plugging in different household scenarios to see what actual, real world price hikes look like.
Throughout all of these examples, however, two things have remained consistent:
In yesterday's write-up about CMS posting the first official, state-by-state data breakout for the ongoing 2026 ACA Open Enrollment Period, I noted several possible reasons why so far enrollment is running a solid 11% ahead of the same point a year ago even with widespread knowledge of the enhanced federal tax credits expiring just 25 days from now:
Total 2025 enrollment was 13.4% higher than total 2024 enrollment; assuming a similar rate of net attrition over the course of the year, there should be around 13% more current enrollees who can potentially actively renew/re-enroll for 2026 to begin with. As it happens, re-enrollment is currently up around 14% over the same point a year ago.
There's been a MASSIVE amount of attention given to the ACA, the exchanges, Open Enrollment, etc etc this year due to the panicky headlines about the impending subsidy expiration and of course the 43-day long federal government shutdown which focused primarily on...the ACA, the exchanges, Open Enrollment and the impending subsidy expiration.
The Centers for Medicare & Medicaid Services (CMS) reports that nearly 950,000 consumers who do not currently have health care coverage through plans in the individual market Marketplace have signed up for coverage in 2026, since the start of the Marketplace Open Enrollment Period (OEP) on November 1, 2025. Existing consumers are also returning to the Marketplace to actively renew their coverage, and anyone who does not actively renew will be automatically re-enrolled for 2026. Over 4.8 million existing consumers have already returned to the Marketplace to select a plan for 2026.
Definitions and details on the data in this report are included in the glossary.
As usual, I'll start out with the top line numbers, compared to the same point last year:
On Get Covered Colorado Day, Connect for Health Colorado and state leaders urge customers to compare options and maintain health coverage in 2026.
Denver, Colo.– Today is Get Covered Colorado Day, a day of action designed to encourage as many Coloradans as possible to enroll in 2026 health insurance during Connect for Health Colorado's annual open enrollment period.
“Our message today is simple: we’re here to help every Coloradan get covered,” said Kevin Patterson, chief executive officer of Connect for Health Colorado, the state’s official health insurance marketplace. “Even with premium increases and the possible expiration of federal enhanced Premium Tax Credits, Coloradans are finding plans that fit their needs and their budgets – and they’re not doing it alone. Our experts are ready to guide customers every step of the way. We want Coloradans to know there’s no better time than now to shop, compare options and take advantage of the support we have available.”
There are 43 U.S. House districts where the Republican nominee won by 15 points or less. Of those, one (WA-04) doesn't really count since there were 2 Republicans running in the general election (Washington State has "jungle primaries"). Four others were won by Donald Trump by between 16 - 20 points (AZ-08, CO-04, TX-15 & WI-08).
That leaves 38 GOP-held House seats where the Republican won by 15 pts or less and where either Kamala Harris won, or Donald Trump also won by 15 points or less. The table below breaks these out with both margins, while also listing my estimate of how many residents of each district are enrolled in ACA coverage.
To: Plymouth Union Public Advocacy From: Tony Fabrizio & Bob Ward
Date: July 14, 2025
Re: Expiration of Premium Tax Credits Survey – Targeted Congressional Districts
Our survey of voters in the most competitive Congressional Districts shows Republicans have an opportunity to overcome a current generic ballot deficit and take the lead by extending the healthcare premium tax credits for those who purchase health insurance for themselves. Without Congressional action, the tax credit expires this year.
For 12 years now, one of the traditions of ACA Signups has been The Graph: A line graph tracking enrollment in ACA policies over the course of each Open Enrollment Period.
The original Graph from 2013-2014 looked quite different from more recent years, partly because I was attempting to track Medicaid/CHIP enrollment and other coverage categories at the same time, and partly because, frankly, I didn't really know what I was doing at the time.
Over the next few years I modified & improved both my methodology as well as the format, culminating in last year's 2025 Open Enrollment Period Graph, which featured the highest enrollment figures in the ACA's history: ~24.3 million Qualified Health Plan (QHP) enrollees, plus another ~1.8 million Basic Health Plan (BHP) enrollees in Minnesota, New York & Oregon specifically, for a grand total of just a hair over 26 million people.
For the 2026 Open Enrollment Period, however, actual hard enrollment data has been, shall we say, difficult to come by so far.
I don't know if this is new or not, but it turns out that Covered California--the largest state-based ACA exchange in the country--has an Open Enrollment Dashboard after all!
This means that in addition to two small states regularly reporting Open Enrollment data (Maine and New Mexico), the largest one is as well!
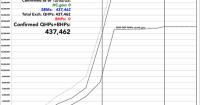
Here's what Covered CA is reporting as of November 29th:
New enrollments: 45,023
Active renewals: 365,879
Passive/Autorenewals: 1,412,526
Total: 1,823,428
As I've noted in both my Maine and New Mexico updates, while I include the passive/auto-renewal number for completeness sake, that number won't really be relevant until after the deadline for January 1st coverage passes (which is December 15th in most states, although not until 12/23 in MA & 12/31 in MD, NV, NJ, NM & RI).4,