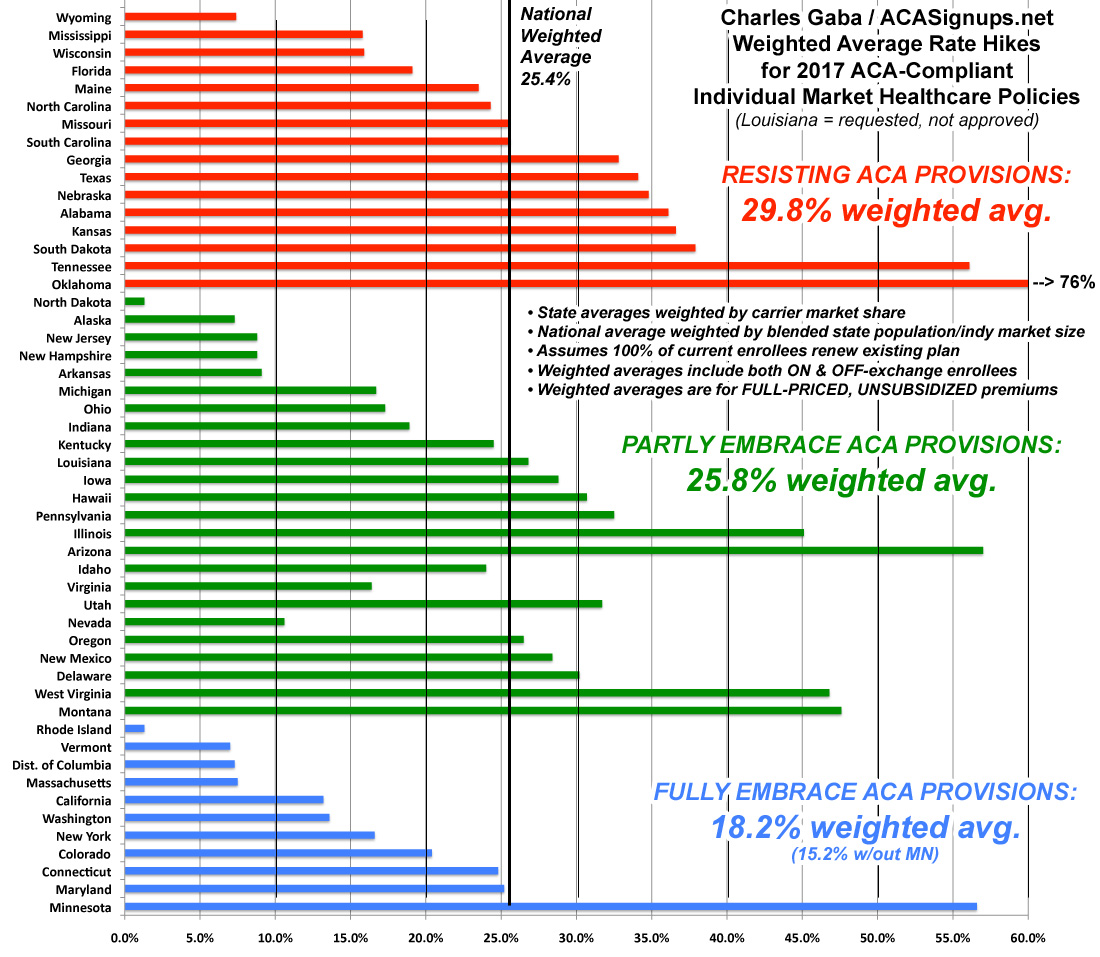
The states which are 100% on board with the ACA exchange provisions (running their own full state-based marketplace, expanding Medicaid and sticking to the original cut-off date for "transitional" policies) average around 18%. If you remove Minnesota from the equation, it's just 15.2%.
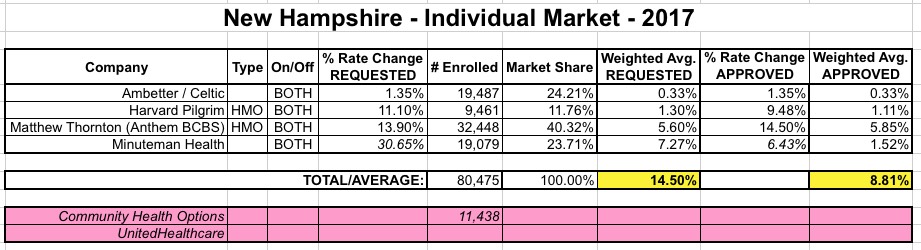
(sigh) OK, with three states still missing, you just knew I wouldn't rest until I was able to fill in the missing pieces of the puzzle. Sometime today, the HHS Dept. finally entered the approved rate hikes for individual makret carriers in two of those states: New Hampshire and Virginia. Louisiana is still AWOL for whatever reason.
It's important to note that sometimes the "Final Rate Increase" percentages listed at RateReview.HealthCare.Gov dont' actually end up matching the approved rate hikes found in the official SERFF databases or even at the state's Dept. of Insurance website. Normally I cross-check all three to make sure nothing weird is going on, but given that it's well past time to move on, I'm relying purely on the RateReview numbers for these states.
With that in mind, here's what it looks like in each:
Now it looks like another projection of mine is gonna be proven (unfortunately) accurate.
A week and a half ago, the HHS Dept. confirmed that as of the end of the 2nd quarter (June 30), there were about 10.5 million people still enrolled in effectuated QHPs via the ACA exchanges. As I noted at the time, this was about 300,000 fewer people than I had assumed would be enrolled at that point, so I revised my projections for the second half of the year:
I assumed a similar pattern to last year, with roughly 15% net attrition as of the end of June, which would have resulted in roughly 10.8 million people having effectuated exchange policies as of 6/30/16. Instead, they say it was around 10.5 million. Based on this new data, I'm revising my net attrition estimates for the rest of the year to perhaps 9.8 million as of the end of September. If so, this would result in ending 2016 with around 9.2 million people enrolled in effectuated exchange policies, for a 2nd-half monthly average of around 9.9 million and a full-year monthly average of around 10.1 million.
The main focus of this Late Night with Seth Meyers segment is about how Donald Trump completely whiffed on what should have been a reasonably strong attack on Hillary Clinton: Namely, the 25% average unsubsidized individual market rate hikes which are coming next year.
In the process, however, Meyers actually did a fairly good job of summarizing the situation:
"Now, that's bad news on the surface...but it's still in line with the projections made by the Congressional Budget Office. Obviously, Obamacare is a nuanced, complicated issue that requires sober analysis and discussion...or, as Donald Trump put it..."
NOTE 10/29/16: For anyone who read this entry yesterday, please note that I've gone back and completely reworked all 4 the charts, along with adding a fifth one, for several reasons:
I had to correct an error re. Medicaid expansion (I had Iowa not expanded and Wisconsin expanded by mistake)
I was able to add the final approved averages for both New Hampshire and Virginia, leaving Louisiana as the only state with a "requested" average only
The original graphs only listed the median rate hikes for each group; they now list the actual weightedaverages for each group of states
I even added a fifth chart which separates the states out into those which embraced all 3 provisions vs. those which only embraced 1 or 2 of them, and those which didn't implement any.
OK. I ran the numbers several different ways way back in August, when I had compiled the requested 2017 individual market rate hike averages for all 50 states (+DC). However, many things have changed since then. Not only do I have the approved rate changes for 48 states, there were a lot of other major changes along the way, including various carrier pullouts and rate filing re-submissions.
As noted before, I'm really trying to move onto the actual enrollment part of the 2017 open enrollment period, but I can't resist doing some more final cleanup of my Rate Hike project:
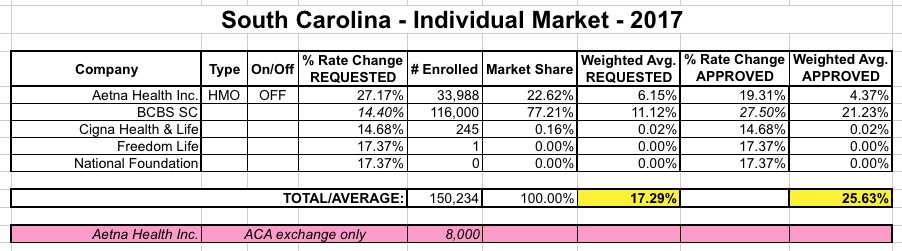
SOUTH CAROLINA: This is one of the 5 states which I still didn't have approved rate changes for. Today the RateReview.HC.gov site finally added in the final numbers for SC, so here's what it looks like:
Aetna was a bit tricky--the total enrollee number is actually 41,988. They dropped out of the ACA exchange but are sticking around the off-exchange market, so I had to figure out how many of those 42K are on vs. off-exchange. The answer is in this article which notes:
More than 220,000 South Carolinians rely on the federal health care law for insurance. This year, only 8,000 of them are covered by Aetna plans.
Donald Trump on Tuesday claimed that the Obama administration is lying about the size of ObamaCare premium hikes, saying it put out a "phony" number.
The administration on Monday announced that the average premium increase for a benchmark ObamaCare plan will be 25 percent for 2017, a number seized on by Republicans.
But Trump took the line of attack a step farther.
“And the number of 25 percent is nothing,” the GOP presidential nominee told Fox News. “That’s a phony number, too, that’s a lie, just like everything else.”
Going into the fourth year of open enrollment, my work here at ACA Signups has started to fall into a seasonal pattern. During open enrollment itself, of course, it's all about the core mission of the site: Live-tracking the number of people who actually sign up for ACA exchange policies, and the related news items which accompany that. In the spring, it's all about dust settling and wrapping up: Plugging in the hard numbers, seeing how they compare with what I had projected and so on.
In the summer and fall, however, I'm on my second year of tracking the average (unsubsidized) rate increases people can expect for the following year.
Last week I noted that with 41 states accounted for and the 2017 Open Enrollment Period quickly bearing down on everyone, it was time to pull the plug on my 2017 Average Rate Hike project and move on. I had come up with an overall national weighted unsubsidized average rate increase of around 25% for ACA-compliant individual market plans.
However, I also noted that I'd make sure to fill in the approved rates for the remaining 10 states as they came in, for completeness sake...and today, thanks to the HHS Dept. cutting the ribbon on 2017 Window Shopping at HealthCare.Gov, I've also been able to fill in the blanks for five of the remaining states all in one shot (the other five remain elusive).