Vermont is the fourth state to announce their approved 2020 ACA individual/small group market premium rate changes. VT (along with Massachusetts and DC) has (wisely, in my opinion) merged the risk pools for the two markets into one, meaning I have to plug the numbers in differently on my spreadsheet.
Back in mid-May, my initial analysis of the two carriers participating in both Vermont markets put the weighted average rate increase being requested at an even 13.0% statewide: Blue Cross Blue Shield of VT was requesting a 15.6% increase, while MVP Health Care asked for a 9.4% bump.
Back on May 31st, I reported that New York's Dept. of Financial Services had released the preliminary, requested premium rate hikes for the 2020 ACA individual and small group markets. At the time, the weighted average increase requested state-wide was around 8.4% (although I got 8.3% when I plugged the hard enrollment numbers into a spreadsheet).
For the small grouip market, NY DFS reported an average requested increase of 12.0%, although again, I only got 11.3% when I plugged in the numbers.
Yesterday, however, NY DFS became the third state (after Oregon and Virginia) to publicly release their approved 2020 premium changes...and like OR & VA, they've shaved a few points off the average rates:
DFS ANNOUNCES 2020 PREMIUM RATES: LOWERS OVERALL REQUESTED RATES FOR INDIVIDUALS AND SMALL BUSINESSES TO PROTECT CONSUMERS AND FUEL A COMPETITIVE HEALTH INSURANCE MARKETPLACE
At long last, I've completed my analysis of the preliminary 2020 rate filings for ACA-compliant individual market policies across all 50 states (+DC)! in most cases I've also included the small group market, although with far less documentation for those.
Texas, understandably enough, has the third largest individual market in the country after California and Florida, at somewhere around 1.27 million enrollees (they had around 990,000 on-exchange enrollees; I'm pretty sure around 75% of the market is on-exchange these days).
There's ten carriers offering ACA policies on the individual market in Texas, and fifteen participating in the small group market. Unfortunately, most of the rate filings are redacted or missing data altogether (again), so I was only able to cobble together hard enrollment data for half the Indy market carriers, comprising just 15% of the statewide market. I've run an unweighted average for the other five carriers, and blended that with the first five for a semi-weighted average rate hike of just 0.8% overall.
I know this is an imperfect way of doing it, but it's the best I can do at the moment. I hope to have more complete data once the approved filings are made available.
New Jersey is an important state to watch, as they (along with DC) are the first state to specifically reinstate the ACA individual mandate penalty at the exact same levels as the just-zeroed out federal version. Massachusetts has a mandate penalty in place this year as well, but a) theirs pre-dated the ACA and was simply dusted off again and b) theirs uses a different formula anyway.
Last year, Individual Market insurance carriers in New Jersey announced that average unsubsidized 2019 premiums would be reduced by an average of 9.3% statewide due to two laws put into place by the state legislature and Governor Murphy: Reinstatement of the mandate penalty at federal levels (which lowered rates by 6.8 percentage points from +12.6% to just +5.8%) and the initiation of a solid reinsurance waiver program (which reduced rates by a further 15.1 points, for a final average change of -9.3%).
Unfortunately, North Dakota is another state where the carriers have redacted their rate filings. I was able to garner some info about one of the three carriers participating in the Individual Market next year: Medica's filing redaction wasn't done properly, so I was able to extract that they're looking at medical trend of 7.7%, a morbidity reduction of 1.5%, a 2.3% increase due to the reinstatement of the ACA's insurer fee...and a 20% reduction due to the implementation of the state's reinsurance program, which I first reported on last fall and followed up with this spring.
(sigh) I'm into the home stretch with only a handful of states left to go. Unfortunately, South Carolina is yet another state where the actual enrollment numbers are either missing or redacted, making it impossible to run a properly weighted average...but again, the range between the three carriers offering individual market policies is so narrow that it doesn't make much difference anyway (between -3.72% and +0.17%).
The unweighted average is a 1.9% reduction in unsubsidized premiums statewide.
On the small group market, however, average 2020 premiums are jumping by double digits: 11.1%.
David Balat is the director of the Right on Healthcare initiative at the Texas Public Policy Foundation, a conservative think tank which pushes school vouchers and which attempts--against all sanity--to claim there's a moral case in favor of fossil fuels, which I guess should be described as "natural gaslighting."
Anyway, the other day, Mr. Balat posted an op-ed at The Hill in which he tries to gaslight America regarding the lengthy list of ACA sabotage efforts which have been (and which continue to be) pushed by the Trump Administration, some more successfully than others.
Repeated claims of sabotage of the ACA by the Trump Administration fall flat because of these important initiatives put in place by the president. Although the president has chosen to not defend the ACA in the Texas v. Azar case, he has made numerous strides to make available options to help Americans who require coverage suited to their needs, as well as help for those with chronic conditions.
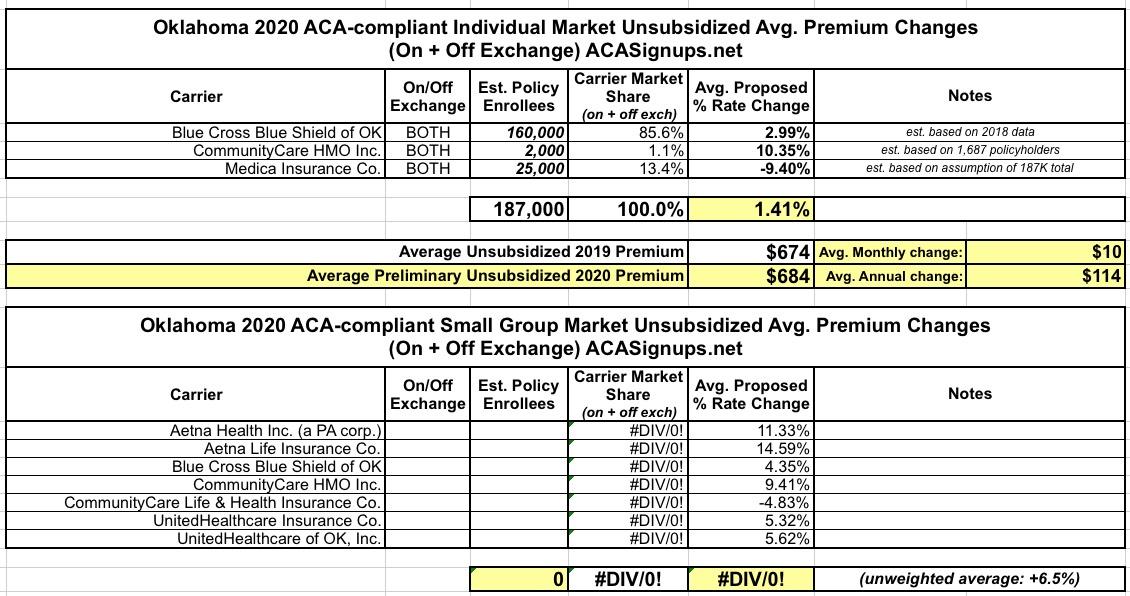
Oklahoma has three carriers on the Individual Market these days. Once again, all three rate filing memos are redacted, but I was able to dig up the number of current policy holders for one of them (CommunityCare HMO).
I've bumped that number up a bit to account for the total number of covered lives to an even 2,000. For the other two carriers, I'm assuming Blue Cross Blue Shield still holds the lion's share of enrollees and that the total on+off-exchange market is around 187,000 people.
If this is all correct, the weighted average rate increase for unsubsidized enrollees is around 1.4% statewide.
Meanwhile, the unweighted average rate hike for the small group market is 6.5%.
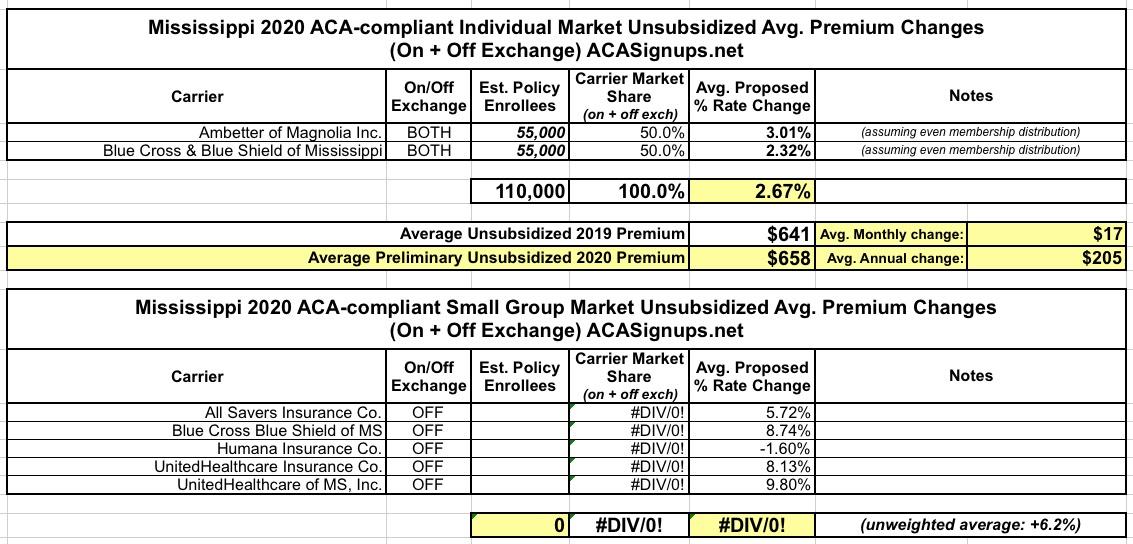
As a result, I have no idea what the relative market share is between the two and am assuming they're roughly even. Even if they aren't, the requested rate changes are so close it doesn't make much difference anyway (2.3% and 3.0%). If approved as is, unsubsidized Mississippians can expect to pay about $200 more total next year.
On the small group market, there's five carriers; again, I don't know the market share of any of them, so the unweighted average increase is 6.2% statewide.
Sen. Lindsey Graham (R-S.C.) said this week that Republicans would push to repeal ObamaCare if they win back the House and President Trump is reelected in 2020.
"If we can get the House back and keep our majority in the Senate, and President Trump wins reelection, I can promise you not only are we going to repeal ObamaCare, we're going to do it in a smart way where South Carolina will be the biggest winner," Graham said in an interview with a South Carolina radio station.
"We've got to remind people that we're not for ObamaCare."
As for "South Carolina will be the biggest winner", he's referring to this, his own "Graham-Cassidy" ACA replacement scheme: