Kris Haltmeyer, a vice president at the Blue Cross Blue Shield Association, told reporters that the premium increases were in part due to the repeal of ObamaCare’s individual mandate in the Republican tax reform bill in December...“With the repeal of the individual mandate and the failure of Congress to enact stabilization legislation, we are expecting premiums to go up substantially,” Haltmeyer said.
...He said the premium increases are “related to the loss of the mandate and then underlying medical costs.”
“Those two things have the most impact on the rate increases,” he added.
...Oh, and what comes after mandate repeal and underlying medical costs? You guessed it: #ShortAssPlans
The Affordable Care Act (ACA), in section 1402, requires insurers who participate in the marketplaces established under that act to offer CSRs to eligible people who purchase silver plans through the marketplaces. CBO views that requirement as establishing an entitlement for thoseeligible.
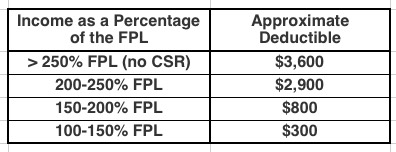
To qualify for CSRs, people must purchase a plan through a marketplace and generally have income between 100 percent and 250 percent of the federal poverty guidelines (also known as the federal poverty level, or FPL). The size of the subsidy varies with income.
CSRs reduce deductibles and other out-of-pocket expenses like copayments. For example, in 2017, by CBOs estimates, the average deductible for a single policyholder (for medical and drug expenses combined) with a silver plan varied according to income in the followingway:
Health Insurance Subsidies and Related Spending.Outlays for health insurance subsidies and related spending are estimated to increase by $10 billion, or 21 percent, in 2018.8 That jump mostly stems from an average increase of 34 percent in premiums for the second-lowest-cost “silver” plan in health insurance marketplaces established under the Affordable Care Act. (Those premiums are the benchmark for determining subsidies for plans obtained through the marketplaces.) Over the 2019–2028 period, the average growth in spending is projected to lessen considerably, to just under 5 percent per year, as per-beneficiary spending rises with the costs of providing medical care. CBO estimates that, under current law, outlays for health insurance subsidies and related spending would rise by about 60 percent over the projection period, increasing from $58 billion in 2018 to $91 billion by 2028.
Yup, thanks to deliberate sabotage from the first two years of the Trump Administration, premiums have spiked by ~30% this year and will do so again next year, requiring federal spending on subsidies to increase accordingly.
The Bipartisan Health Care Stabilization Act of 2018 (BHCSA) would make several changes to health care laws. It would:
Change the state innovation waiver process established by the Affordable Care Act (ACA),
Appropriate a total of $30.5 billion for reinsurance programs or invisible high-risk pools in the nongroup insurance market,
Appropriate funds for the direct payment for cost-sharing reductions (CSRs) through 2021,
Allow any enrollee in the nongroup market to purchase a catastrophic plan, and
Require some existing funding for operations in the health insurance marketplaces to be used specifically for outreach and enrollment activities in 2019 and 2020.
Last week the Congressional Budget Office reported that funding the CHIP program for 5 years, which they had previously estimated would increase the federal deficit by about $8 billion over the next decade, would instead only increase it by about 1/10th as much: Roughly $800 million, a rounding error when it comes to the federal budget. The reason for this isn't that funding CHIP had suddenly become less expensive, it was instead, ironically, because due to the GOP repealing the ACA's individual mandate starting in 2019, NOT funding CHIP has suddenly become more expensive.
All eyes are on the Godawful Tax Scam Bill this week, which once again lies mostly in the hands of a handful of Republican Senators including the usual suspects like John McCain, Lisa Murkwoski and Susan Collins.
McCain's biggest beef this year has been about "following regular order"; it's the reason he shot down the GOP's #BCRAP bill last summer. Of coruse, current tax bill most certainly isn't following regular order either. Will he stick to his guns on the issue or cave under pressure this time? Who knows?
A few days ago I noted that I had seriously misunderstood the Congressional Budget Office's individual market premium projections in the event the ACA's individual mandate is repealed: Yes, it'd be ugly, but not nearly as bad as I thought, although they still expect up to 13 million people to lose coverage as a result.
Yesterday, the Center for American Progress did an analysis which broke out those 13 million by state...along with the impact on individual market premiums and the 25 billion in immediate Medicare cuts which the GOP's tax bill would implement.
While I have my own doubts about some of the CBO's assumptions, there can be no doubt that premiums would increase substantailly, millions of people would end up without healthcare coverage, and the $25 billion in Medicare cuts do appear to be locked in if the GOP's bill were to become law:
Several regular commenters here at ACA Signups have been wondering why the Congressional Budget Office keeps using March 2016 as the "baseline" for projecting the net impact on healthcare coverage numbers under the GOP's Trumpcare bills (the House's AHCA and the Senate's BCRAP), as opposed to the more recent January 2017 baseline. After all, according to the March 2016 baseline, the CBO was projecting that under the ACA, the total individual market would have 25 million people as of 2026 (18 million on the exchanges plus another 7 million off-exchange), whereas under the January 2017 baseline, their projections are for the individual market to only be 20 million as of 2027 (13 million on the exchanges plus 7 million off-exchange). Taken at face value, this would seem to suggest a 5 million enrollee discrepancy. This drumbeat has been taken up more recently by GOP Senators, particularly Wisconsin Senator Ron Johnson.
CBO aims to provide preliminary assessment of Graham-Cassidy bill by early next week
CBO is aiming to provide a preliminary assessment of the Graham-Cassidy bill by early next week. That assessment, which is being prepared with the staff of the Joint Committee on Taxation, will include whether the legislation would reduce on-budget deficits by at least as much as was estimated for H.R. 1628, the American Health Care Act, as passed by the House on May 4, 2017; whether Titles I and II in the legislation would each save at least $1 billion; and whether the bill would increase on-budget deficits in the long term. CBO will provide as much qualitative information as possible about the effects of the legislation, however CBO will not be able to provide point estimates of the effects on the deficit, health insurance coverage, or premiums for at least several weeks.
Well this was unexpected, although I suppose I should have expected it given all the insanity surrounding the impending deadlines for insurance carriers to sign contracts (Sept. 27th, I believe); the end of the fiscal year on Sept. 30th (which is also the last chance for the GOP to try and squeeze through the hideous Cassidy-Graham Hail Mary repeal/replace bill); and the start of Open Enrollment on November 1st.
The CBO has issued a 17-page report with their latest projections for the types of healthcare coverage and federal spending on healthcare programs including Medicaid, CHIP, ACA tax credits and so forth over the next decade. here's what they foresee:
The federal government subsidizes health insurance for most Americans through a variety of programs and tax provisions. In 2017, net subsidies for people under age 65 will total $705 billion, CBO and the staff of the Joint Committee on Taxation (JCT) estimate.