(I know numerous other states with Democratic governors have issued similar executive orders already, but I'm a lifelong Michigander as are most of my family so this one comes as particular relief to me)...
via email (no link yet):
Governor Whitmer Signs Executive Directive, Ensuring Michiganders Can Access Vaccines to Stay Healthy Ahead of Cold, COVID-19, and Flu Season
LANSING, Mich.—Today, Governor Gretchen Whitmer signed an executive directive, ensuring vaccines remain available to Michiganders as we approach the fall. Specifically, she has instructed state agencies to identify and remove any barriers to accessing COVID-19 vaccines, so Michiganders can stay healthy ahead of cold and flu season. Governor Whitmer remains committed to supporting the health and wellbeing of every Michigander and their families.
I just finished writing up a deep dive into the Arkansas Insurance Dept's move from laissez faire-style Silver Loading to fully-regulated & maximized Premium Alignment in an attempt to mitigate the massive net premium damage about to be caused if the enhanced ACA premium tax credits expire at the end of 2025.
However, it's not just Arkansas which has finally seen the light and joined about a dozen other states in putting full-bore Premium Alignment (PA) pricing into place to help reduce the financial burden on ACA individual market enrollees in 2026.
Other states which have already done so in the past include Colorado (sort of), Texas, New Mexico, Maryland, Pennsylvania (somewhat), Illinois, Vermont and Wyoming.
Warning: This isn't just gonna get deeply wonky, it also requires digging deep into hisory. You've been warned.
Chapter 1: The (simplified) Backstory:
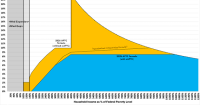
The ACA includes two types of financial subsidies: Advance Premium Tax Credits (APTC), which reduce monthly premiums; and Cost Sharing Reductions (CSR), which cut down on deductibles, co-pays & other out-of-pocket (OOP) expenses for low-income enrollees.
In 2014, then-Speaker of the House John Boehner filed a lawsuit on behalf of Congressional Republicans against the Obama Administration, in part because they claimed that CSR payments were unconstitutional because they weren't explicitly appropriated by Congress in the text of the Affordable Care Act.
A long legal process ensued, the end of which resulted in a federal judge ruling in the GOP's favor and ordering that CSR payments stop being made...but also staying that same order pending appeal of her decision by the Justice Department (then still run by the Obama Administration).
(sigh) So, moments ago I received the following press release from the Centers for Medicare & Medicaid Services (CMS):
Today, the Centers for Medicare & Medicaid Services (CMS) unveiled details on how states can apply to receive funding from the $50 billion Rural Health Transformation Program created under the Working Families Tax Cuts Act to strengthen health care across rural America. This unprecedented investment is designed to empower states to transform the existing rural health care infrastructure and build sustainable health care systems that expand access, enhance quality of care, and improve outcomes for patients.
Amusingly (and sadly), the link itself goes to the WhiteHouse.Gov page describing not the "Working Families Tax Cuts Act" (which doesn't exist) but rather the so-called "One Big Beautiful Bill Act" which is what Trump and Republicans insisted on calling it for months, right up until they realized that it's about as popular as a turd in a punchbowl, at which point they decided that simply rebranding it as a "tax cut" for "working families" will solve all their problems at the midterms next year.
If you've been following my state-by-state 2026 avg. rate change project, you may have noticed that after filling in the final, approved rate filings for a bunch of states over the past month or so, these tapered off to just three more last week (Illinois, Washington and Connecticut).
State Highlights Rising 2026 Health Insurance Rate Proposals
SAINT PAUL, MN: Minnesotans are facing unnecessarily higher health insurance rate hikes, and the blame lies with new Republican-led federal policy changes passed in Washington, says Minnesota Commerce Commissioner Grace Arnold.
“While HR1 has been dubbed the “One Big Beautiful Bill” by Republicans, many in our state will find nothing beautiful in health insurance premium increases they’ll experience for 2026,” Arnold said. “These will be the highest rate hikes since 2017 for individual and group markets.”
The Connecticut Insurance Department has posted the initial proposed health insurance rate filings for the 2026 individual and small group markets. There are 8 filings made by 7 health insurers for plans that currently cover approximately 224,000 people (158,000 individual and 66,000 small group).
Anthem has filed rates for both individual and small group plans that will be marketed through Access Health CT, the state-sponsored health insurance exchange. ConnectiCare Benefits Inc. (CBI) and ConnectiCare Insurance Company, Inc. have filed rates for the individual market on the exchange.
Before I continue, note that yes, I'm aware the 17.8% average shown below doesn't match the 22.9% average in the headline above. There's a reason for this which should be obvious if you read on:
The 2026 rate proposals for the individual and small group market are on average higher than last year:
Last week I noted that Colorado legislators passed (and Gov. Polis signed) legislation to scrape together up to $100 million in emergency funding to backfill perhaps 40% or so of the federal tax credits the state expects their ~225,000 subsidized enrollees to lose in 2026 when the enhanced IRA credits expire this December:
...The Senate then approved House Bill 25B-1006, which would sell tax credits to bring in money for the Health Insurance Affordability Enterprise fund. That pays for programs to reduce individual insurance market premiums.
The bill aims to raise $100 million for that enterprise to soften the impact of the expiration of federal enhanced premium tax credits. Health insurance premiums for people who buy insurance on the individual market are expected to face an average of a 28% increase next year, with higher increases along the Western Slope.
This is gonna be one of the stranger references I've made on this site, but bear with me.
Back in 1996 there was an HBO movie called "The Late Shift" which told the story of the Late Night TV show battle between David Letterman and Jay Leno over who would succeed Johnny Carson as host of The Tonight Show. As stupid as this may sound today, this was actually a Really Big Deal in the '90's...one of those absurd pop culture stories which dominated the headlines and the tabloids for several years.
The movie itself was decent, with some interesting casting including Kathy Bates and Treat Williams, but nothing special. The main problem is that the audience is expected to root and feel sympathy for a couple of dudes who were already rich & famous and who would both continue to be rich & famous no matter how the story played out. The stakes weren't exactly the fate of the world, is what I'm saying.