Japanese holdouts (残留日本兵 Zanryū nipponhei?, "remaining Japanese soldiers") or stragglers were Japanese soldiers in the Pacific Theatre who, after the August 1945 surrender of Japan ending World War II, either adamantly doubted the veracity of the formal surrender due to strong dogmatic or militaristic principles, or simply were not aware of it because communications had been cut off by the United States island hopping campaign.
They continued to fight the enemy forces, and later local police, for years after the war was over. Some Japanese holdouts volunteered during the First Indochina War and Indonesian War of Independence, to free Asian colonies from Western control despite these having once been colonial ambitions of Imperial Japan during World War II.
Intelligence officer Hiroo Onoda, who was relieved of duty by his former commanding officer on Lubang Island in thePhilippines in March 1974, and Teruo Nakamura, who was stationed on Morotai Island in Indonesia and surrendered in December 1974, were the last confirmed holdouts, though rumors persisted of others.
Since the Supreme Court has ensured the viability the federally-facilitated exchanges, they could be the best option for other states with problematic marketplaces. “There is no new money now to build new infrastructure, and there are no grants available to fix these systems if they’re struggling,” said Heather Howard, the director of the Princeton University program that advises states on exchange building, told the Times. “So the only path forward may be to use HealthCare.gov.”
Did Obama Cover Up Real Reason for Obamacare Website Crash?
Nearly two years after its failed launch, there still remain more questions than answers, but perhaps the recent King v. Burwell case has subtly lifted the veil on the real reason for the crash.
Hmmmm..."subtly lifted the veil"? I'm intrigued! Do go on...
At the time of the HealthCare.gov crash, Obama’s media spin doctors insisted the site’s failure was caused by “extremely high” traffic, as Sebelius reiterated in an interview with CNN’s Sanjay Gupta. According to Sebelius, nearly 20 million people visited the site in just the first three weeks, a volume site designers simply weren’t prepared for.
Anyone over the age of 40 or so--regardless of their political stripes--should demand that, henceforth, July 12 be given the same Unofficial National Holiday status that, say, Star Wars Day has received.
A few weeks ago I reported that Indiana's implentation of the ACA's Medicaid expansion provision, which kicked off at the end of January, was already up to 237,000 enrollees.
Industry representatives say Indiana's expanded health care program for low-income residents has functioned smoothly in the months since it was implemented following federal approval.
The federal Centers for Medicare and Medicaid Services in January approved expanding the existing Healthy Indiana Plan into a larger program that Gov. Mike Pence has dubbed HIP 2.0. That program uses federal Medicaid funds under President Barack Obama's health care law to cover people with incomes under 138 percent of the federal poverty level.
State enrollment in HIP 2.0 has climbed to nearly 290,000 participants, with about 60 percent of those people under age 40, according to state figures presented Thursday during a public hearing in Indianapolis on the program.
For the first time, the Obama administration has deployed an important new power it has under the Affordable Care Act: proposing to pay doctors and hospitals based on the quality of care they provide, regardless of whether they want to be paid that way.
It rolled out two such programs this week. One would require all hospitals in 75 metropolitan areasto accept a flat fee for the costs associated with a hip or knee replacement — including the costs of surgery, medications, the joint implant and rehabilitation. And if the quality of the care is not judged to be good, Medicare will take back some of the money it paid. Another program would increase or decrease payments tohome health agencies in nine states, depending on how they perform on certain quality measurements.
This story is mainly included for reference if/when I'm able to do a market share/rate increase analysis of Illinois in the future:
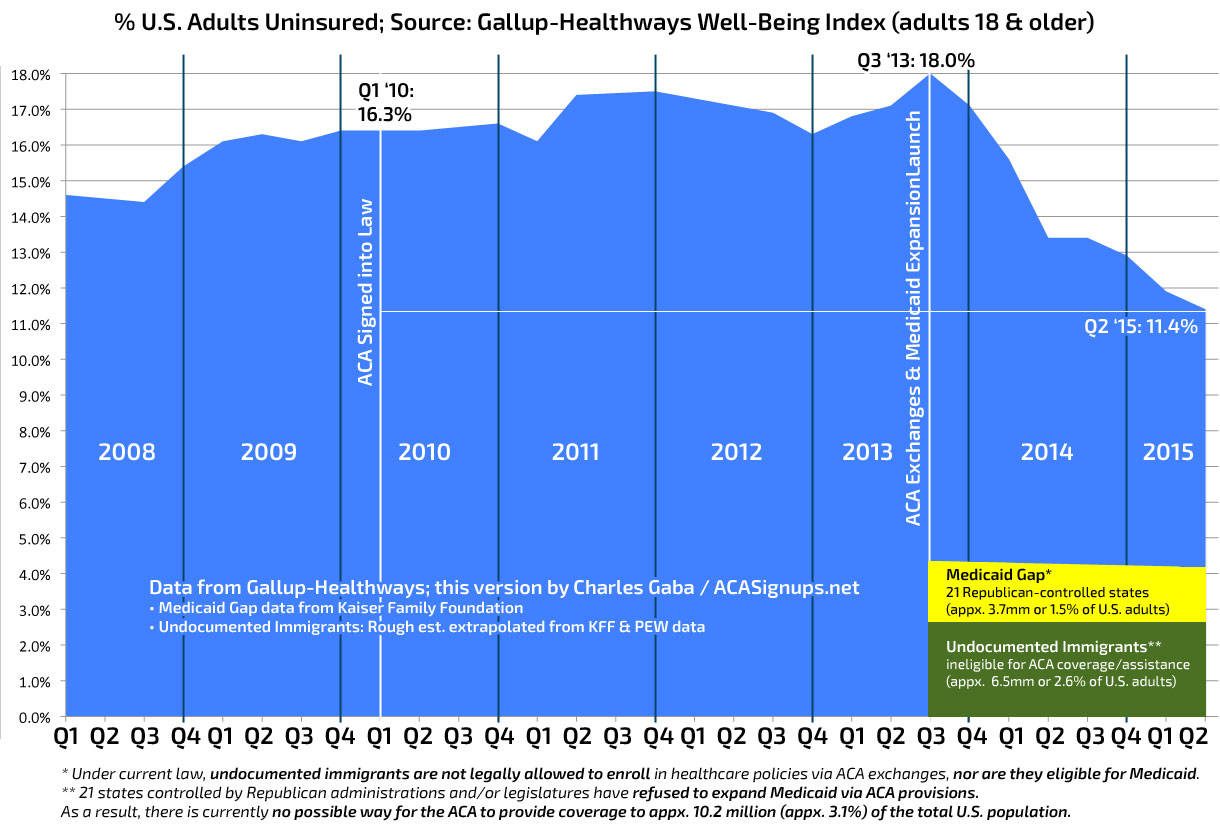
Yesterday, after the big quarterly Gallup survey was released showing a total reduction in the uninsured among U.S. adults from 18% in October 2013 down to 11.4% in June 2015, I went ahead and whipped up a more detailed graph which 1) includes the full range starting from 0% (Gallup's official graph cuts off the first 10%, which gives a bit of a false impression of the true situation); 2) includes the 2 key dates: March 2010 (when the ACA was signed into law) and October 2013 (when the ACA exchanges/Medicaid expansion enrollments started); and 3) also includes 2 extremely important color-coded areas: The 3.7 million people caught in the "Medicaid Gap" in 21 Republican-controlled states, and the millions of uninsured, undocumented immigrants nationwide.
Just 3 days ago, I wrote about the changing 2016 rate increase request situation in Connecticut, where Arielle Levin Becker reported that 2 of the state insurance providers were lowering their requested rates ahead of the public regulatory hearings...even though the CT exchange, Access Health CT, is increasing their rates a bit to cover expenses. As a result, the overall weighted average increases being requested dropped a half a point, from 7.7% down to 7.2%, which is pretty darned good, all things considered.
The four companies selling individual health plans through Connecticut’s health insurance exchange have revised their proposals to raise rates in 2016, seeking lower increases than initially proposed.
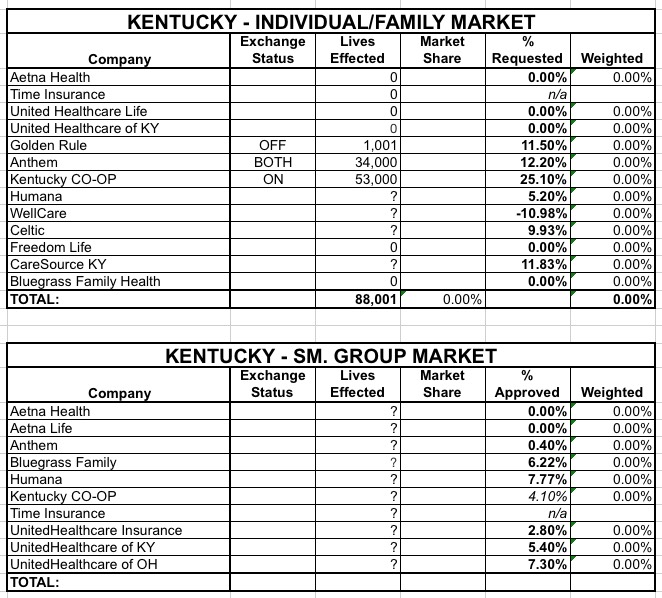
Last week Oregon became the first state to actually approve their 2016 individual/family and small group market policy rate changes. Yesterday, Kentucky appears to have become the second:
Unfortunately, as you can see, while the average rate request for each company is listed, it isn't easy to find the actual enrollment/market share data for most of them, making it impossible to get a weighted average. In addition, there's an awful lot of "n/a / 0%" entries for some pretty big companies. Usually this means that they're new to the market, but I'm not sure that's the case here.
Anyway, assuming that I have the partial data above accurate, it looks like Kentucky's individual market changes will range from an 11% decrease (for WellCare Health Plans of Kentucky, Inc.) to a wince-inducing 25% increase (for the Kentucky Health CO-OP). I don't know how many are enrolled in WellCare right now, but the CO-OP has 53,000 customers, so expect some shuffling around...except, again, I have no idea what that's a 25.1% increase from.
Breaking: Birth Control Coverage Guaranteed for All — Despite Religious Exemptions
Now free coverage of all forms of birth control is guaranteed for all women, no matter where they work. The Obama administration on Friday issued a workaround to last year’s Hobby Lobby ruling, which gave companies religious exemptions on coverage for certain forms of birth control.