HOWEVER, the MLR rule is still pretty important...and while the dollar amounts I'm about to discuss aren't much more than a rounding error in terms of federal budget numbers, it's possible that the could play a small role in helping get a much larger project moving forward.
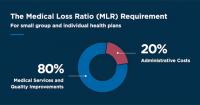
Before I begin, here's a short refresher on how the MLR rule works:
For over a year, I've been tracking the rates of both COVID-19 vaccinations as well as COVID-19 cases & deaths, broken out by county-level partisan lean (namely, what percent of the vote Donald Trump received in 2020).
I've received quite a bit of attention for these analyses, including several national media outlets which have used my work (sometimes with proper attribution, sometimes without) However, there have also been numerous critics who have pointed out that I don't run multivariate analysis when I do this.
Put simply, I look at the correlation between partisan lean and COVID death/vaccination rates or between vaccination rates and COVID death rates...but I don't include other factors like age, income, race/ethnicity, urban-rural status, employment status, health insurance status and so forth.
States will have an additional year to use American Rescue Plan funds to strengthen the home care workforce and expand access to services
Today, the U.S. Department of Health and Human Services (HHS), through the Centers for Medicare & Medicaid Services (CMS), is notifying states that they now have an additional year — through March 31, 2025 — to use funding made available by the American Rescue Plan (ARP) to enhance, expand, and strengthen home- and community-based services (HCBS) for people with Medicaid who need long-term services and supports. This policy update marks the latest action by the Biden-Harris Administration to strengthen the health care workforce, help people receive care in the setting of their choice, and reduce unnecessary reliance on institutional care.
Regular readers may have noticed that I barely posted anything on the site last week, with good reason: I was out of town. I drove out to DC for a few days, ostensibly to attend the annual National Institute of Health Care Media (NIHCM) Awards Dinner, where I was a finalist in the Digital Media category this year.
(I didn't win, but that's OK...the competition was extremely impressive and it really was an honor just to be nominated, really!)
This was the fifth time I've visited the nation's capital, but the first time that I've driven. It's also the first road trip I've taken in an electric car, a brand-new 2022 Kia Niro EV (it replaced my 17-year-old Hyundai which was so badly rusted underneath that my mechanic was surprised it survived the past winter).
I don't often post blog entries about non-healthcare related issues, but I've had a lot of folks express curiosity about what it's like owning/driving an EV in the real world, so I figured this trip (which was, after all, for a healthcare awards dinner, and I also had healthcare policy meetings with a couple of folks on Capitol Hill) would be a good case study to give some thoughts on the subject.
Today, the U.S. Department of Health and Human Services (HHS) through the Centers for Medicare & Medicaid Services (CMS) approved California, Florida, Kentucky, and Oregon actions to expand Medicaid and Children’s Health Insurance Program (CHIP) coverage to 12 months postpartum for a total of an additional 126,000 families across their states, annually—supporting 57,000; 52,000; 10,000; and 7,000 parents, respectively.
via the Centers for Medicare & Medicaid Services (CMS), by email:
Today, the Centers for Medicare & Medicaid Services (CMS) released the latest enrollment figures for Medicare, Medicaid, and the Children’s Health Insurance Program (CHIP). These programs serve as key connectors to care for more millions of Americans.
Medicare
As of February 2022, over 64.2M people are enrolled in Medicare. This is a decrease of 6K since the last report.
34.9M are enrolled in Original Medicare.
29.4M are enrolled in Medicare Advantage or other health plans. This includes enrollment in Medicare Advantage plans with and without prescription drug coverage.
49.9M are enrolled in Medicare Part D. This includes enrollment in stand-alone prescription drug plans as well as Medicare Advantage plans that offer prescription drug coverage.
Over 11.9 million individuals are dually eligible for Medicare and Medicaid, so are counted in the enrollment figures for both programs.
Almost exactly ten years ago, in the federal National Federation of Independent Business v. Sebelius case which was the first of several high-profile federal lawsuits which attempted to eliminate or cripple the Patient Protection & Affordable Care Act, the U.S. Supreme Court spared the ACA...mostly:
The Supreme Court, in an opinion written by the Chief Justice, John Roberts, upheld by a vote of 5–4 the individual mandate to buy health insurance as a constitutional exercise of Congress's Taxing and Spending Clause (taxing power). A majority of the justices, including Roberts, agreed that the individual mandate was not a proper use of Congress's Commerce Clause or Necessary and Proper Clause powers, although they did not join in a single opinion. A majority of the justices also agreed that another challenged provision of the Act, a significant expansion of Medicaid, was not a valid exercise of Congress's spending power, as it would coerce states to either accept the expansion or risk losing existing Medicaid funding.
Fourteen insurers request average 7.16% rate increase for 2023 individual health insurance market
OLYMPIA, Wash. – Fourteen health insurers filed an average requested rate increase of 7.16% for Washington's individual health insurance market. The plans and proposed rates are currently under review and final decisions will be made this fall.
"More than two hundred thousand people in Washington state get their health coverage through our individual market,” said Insurance Commissioner Mike Kreidler. “It’s critical they have choices for meaningful and affordable coverage. Fourteen insurers have filed plans for next year, and while the choices vary depending on where you live, our market is thriving. I know that premiums and cost-sharing are still high for many, especially those who don’t qualify for subsidies, and we need to do more to address the underlying costs drivers of health care.”
Salem – Oregon consumers can get a first look at requested rates for 2023 individual and small group health insurance plans, the Oregon Department of Consumer and Business Services announced today.
In the individual market, six companies submitted rate change requests ranging from an average 2.3 percent to 12.6 percent increase, for a weighted average increase of 6.7 percent. In the small group market, nine companies submitted rate change requests ranging from an average 0 percent to 11.6 percent increase, for a weighted average increase of 6.9 percent. Our initial review has found that insurers have identified inflation, medical trend, and enrollment changes as factors in the proposed increases. See the attached chart for the full list of rate change requests.
Health Carriers Propose Affordable Care Act Premium Rates for 2023
Public Invited to Submit Comments
BALTIMORE – The Maryland Insurance Administration (MIA) has received the rate filings containing the proposed 2023 premium rates for Affordable Care Act (ACA) products offered by health and dental carriers in the Individual, Non-Medigap (INM) and Small Group (SG) markets.
The carriers’ requested increases are reviewed by the MIA and rates must be approved by the Commissioner before they can be used. Before approval, all filings undergo a comprehensive review of the carriers’ analyses and assumptions. By law, the Commissioner must disapprove or modify any proposed premium rates that appear to be excessive or inadequate in relationship to the benefits offered, or are unfairly discriminatory. The MIA will hold a public hearing on the ACA proposed rates in July and expects to issue decisions in September 2022.