Note: Huge props to Amy Lotven for breaking this story.
I've written about the CSR Saga so many times that I'm getting tired of explaining the backstory. However, once again, here's the short version:
Once again, the very short version is this:
The contract insurance carriers sign when they offer policies on the ACA exchanges is to cover a chunk of low-income enrollee deductibles, co-pays and other out-of-pocket costs which would normally be the enrollees' responsibility. These are called Cost Sharing Reductions (CSR).
The carriers then submit their CSR invoices to the federal government, which is supposed to reimburse the insurance carriers every month.
Donald Trump cut off contrctually-required CSR reimbursement payments to insurance carriers in October 2017...and hasn't made any payments since.
(I'm not going to rehash how Trump was able to cut off those payments with a Thanos-like snap of his fingers; suffice to say it's connected to a lawsuit filed so long ago that John friggin' Boehner was still Speaker of the House at the time).
Back in early December, I noted that while I applauded both New Jersey and the District of Columbia for creating their own individual healthcare coverage responsibility requirements (aka, The Individual Mandate) in response to Congressional Republicans repealing the ACA's federal penalty, doing so also required making sure that residents of NJ/DC *knew* they had done so:
There's only one problem with this: The impact of the mandate penalty is completely psychological in nature. It only works (to the extent that it does at all) if people know that they'll be penalized financially for not complying with the mandate.
I still expect the final national QHP selection tally to increase by around 35,000 more when the dust settles, including perhaps 1,000 more from DC, 5K - 10K more from New York and around 28,000 from Vermont (which hasn't reported anything so far this Open Enrollment Period). If so, the official total should end up around 11.47 million nationally, with the 12 State-Based exchanges coming in around 1.6% higher than last year (an all-time high for them collectively) vs. the 39 states on the federal exchange, which dropped another 3.8% this year. Nationally, the official total should end up around 280,000 enrollees short of last year.
Since then I've plugged in the final numbers from New York (which indeed added around 6,700 more enrollees), the District of Columbia (which added over 3,000 more) and, just this morning, Vermont (which only added 25,000 more, with a caveat). Net increase? 34,889 QHP selections.
That indeed brings the grand total to 11,465,327 QHP selections nationally...or 11.47 million...with the state-based exchanges increasing 1.6% year over year, and the national total dropping 285,000 enrollees.
UPDATE: The final, official CMS enrollment report came out in late April, and there's some minor discrepancies in a few states (especially Minnesota). Nationally, the official total is around 22,000 fewer than I thought. The table below has been updated to reflect this. The state-based exchanges still increased enrollment over last year, but only by 0.9%; nationally, enrollment dropped by 306,000 people.
At long last, the final piece of the puzzle can be added: I just received the final 2019 Open Enrollment Period numbers from Vermont Health Connect.
Before looking at it, it's important to understand that Vermont has a unique way of reporting ACA-compliant healthcare policy enrollments.
For the first two years of Open Enrollment, the state didn't allow any off-exchange (or "direct") enrollments for the individual market (or the small business market, I believe). That means all indy market enrollments were done through the exchange. Due to technical problems (and possibly for other reasons as well), however, starting in 2016 they started allowing direct/off-exchange enrollment as well, as every other state does (the District of Columbia is the only other ACA exchange which has no off-exchange market). However, Vermont still requires the insurance carriers to report those off-exchange enrollees to them and they report them as well.
I wish every state reported their enrollment data this way; it would make it much easier for me to do my job, since as it stands the off-exchange market is a bit of a mystery in most states.
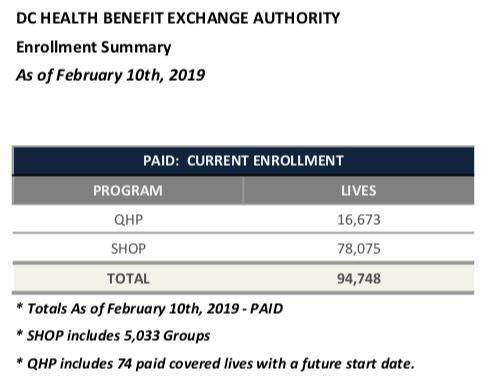
Until now, I've been missing the final 2019 Open Enrollment Period numbers for two state-based exchanges: Vermont and the District of Columbia. VT is still radio silent, but last night the DC exchange authority held their monthly meeting and released their latest data report.
There's a bunch of handy demographic data included in the report...but some of it is also confusing and difficult to get an accurate year-over-year measurement due to a difference of time periods and enrollment status.
I've put in a request to sort some of this out and will update this entry if/when I receive clarification.
For instance, the DC exchange says that they have the following number of residents currently effectuated as of February 10th:
The contrast in how a completely Republican-held state government like Utah and a completely Democratic-held state government like New Mexico deal with Medicaid is pretty astonishing.
In Utah, just four months ago the public voted, clearly and unequivocally, to enact a full expansion of Medicaid to all adults earning up to 138% of the Federal Poverty Line...but the GOP state House, Senate and Governor decided to ignore the voters and override their will by cutting the expansion down to a 100% FPL cap, including work requirements, which will cover tens of thousands fewer people while costing the state $50 million more.
In New Mexico, meanwhile, a newly-enabled Democratic trifecta (I believe both houses of the state legislature were already held by Dems, but the Governorship flipped from Republican Susana Martinez to Democrat Michelle Lujan Grisham) has been on a tear in their first month and a half:
Gov. Brian Kemp will ask the Georgia Legislature and the federal government for flexibility to improve access to government-funded health insurance for the state’s poor and middle class.
His administration told The Atlanta Journal-Constitution on Thursday that it will back a measure that seeks two separate federal “waivers” to Medicaid and the Affordable Care Act to tailor new programs to Georgia’s needs.
This sounds potentially promising, but...
...The ACA waiver, which he outlined on the campaign trail, aims to stop premiums on the health insurance exchange market from rising so fast. A second push, which emerged after his election, would raise the possibility of a partial expansion of Medicaid to some of Georgia’s poorest residents.
I noted last week that Congress held not one, not two but three full hearings regarding various ACA-related issues, at which a couple of friends of mine testified (and a couple more were on the other side of the microphone, as sitting members of Congress).
HEARING ON “STRENGTHENING OUR HEALTH CARE SYSTEM: LEGISLATION TO REVERSE ACA SABOTAGE AND ENSURE PRE-EXISTING CONDITIONS PROTECTIONS”
Date: Wednesday, February 13, 2019 - 10:30am
Location: 2322 Rayburn House Office Building
Subcommittees: Health (116th Congress)
The Subcommittee on Health of the Committee on Energy and Commerce held a legislative hearing on Wednesday, February 13, 2019, at 10:30 a.m. in room 2322 of the Rayburn House Office Building. The bills to be the subject of the legislative hearing are as follow:
In September 2018, the New Mexico Office of the Superintendent of Insurance (OSI) and Health Action NM (an advocacy group for universal access to health care) presented details about potential state actions to stabilize the individual market. OSI has the authority to regulate some aspects of the plans, including maximum duration, but they noted that legislation would be needed for other changes, including minimum loss ratios and benefit mandates.
New Mexico’s insurance regulations were amended, effective February 1, 2019, to define short-term plans as nonrenewable, and with terms of no more than three months. The regulations also prohibit insurers from selling a short-term plan to anyone who has had short-term coverage within the previous 12 months.
The full expansion initiative passed last fall, of course, is supposed to cover Utah residents earning up to 138% of the poverty line, or around 150,000 people...without any work requirements.
The bill barreling through the Utah Legislature was “an effort to override the will of the people,” said Matthew Slonaker, the executive director of the Utah Health Policy Project, a nonprofit group that supported the full expansion of Medicaid.
Utah lawmakers, worried that the sales tax increase might not fully cover the costs, are rushing through a bill that would limit the expansion of Medicaid to people with incomes less than or equal to the poverty level, about $12,140 for an individual.
State officials say that the bill, which is estimated to cover 90,000 people, could be on the desk of Gov. Gary R. Herbert, a Republican, in a week or two.