*(Yes, I know, the District of Columbia isn't actually a state, and Vermont's mandate is...well, read on...)
As the 2020 Open Enrollment Period rapidly approaches (it starts November 1st nationwide...except for California, where open enrollment is starting on October 15th), it's time to start getting the word out about some important things to keep in mind this fall.
One of the most critical things to remember for residents of California, the District of Columbia, Massachusetts, New Jersey, Rhode Island and Vermont is that each of these states* has reinstated an individual healthcare coverage mandate law/ordinance to replace the federal ACA mandate penalty which was zeroed out by Congressional Republicans back in December 2017. This means that if you live one one of them, unless you receive an affordability, hardship or other type of acceptable exemption, you'll be charged a financial penalty when you file your state/district taxes for 2020 in spring 2021 if you don't have qualifying healthcare coverage.
In early August, the Nevada Dept. of Insurance posted the state's preliminary 2020 individual market rate changes. The data was a bit incomplete and confusing, but the bottom line is that average unsubsidized 2020 premiums were only expected to increase about 1.0%.
Today they posted the final/approved rate changes, and unlike most states, the overall weighted average will be slightly higher than the original numbers...although only by a hair:
Nevada Division of Insurance reveals approved 2020 Health Insurance Rates
Carson City, NV – The Division of Insurance (‘Division”) has posted the approved 2020 health insurance rates for all plans in the Individual Health Insurance Market at healthrates.doi.nv.gov and encourages consumers to review this information before the Open Enrollment Period begins.
Long-time readers may remember that back in June 2018, the Trump Administration's Justice Dept. threw all precedence, decency and logic out the window by not only refusing to defend against the idiotic "Texas vs. Azar" lawsuit (aka #TexasFoldEm) brought by 20 Republican state Attorneys General...but went even further by actually agreeing with the plaintiffs that the Patient Protection & Affordable Care Act--which is, remember, the federal law of the land which the DoJ is supposed to defend--is unconstitutional.
At the time, there was one strange thing which was buried within the ugly implications of such a complete abdictation of duty by then-U.S. Attorney General Jeff Sessions: While the Trump DoJ did side with the plaintiffs on the case, they split from the plaintiffs as to what they thought the actual "solution" to the "problem" should be.
Not much to see here...in August, the Idaho Insurance Dept. posted their preliminary 2020 average rate changes for the individual & small group markets; they averaged 7.0% and 4.0% increases respectively. Today they've posted the final/approved rates, and the indy numbers have been whittled down ever so slightly:
Back in July, I noted that the Minnesota Commerce Department announced the preliminary 2020 rate changes for carriers on the individual and small group markets. At the time, the weighted average increases were roughly 1.6% and 5.5% respectively, although the enrollment estimates for each carrier were estimates only.
Today, the MN Commerce Dept. announced the approved rates for 2020, and in both markets, they shaved average premiums down a couple of points. Here's the actual Commerce Dept. press release:
Commerce releases 2020 health insurance rates for Minnesota
Minnesota’s individual and small group health insurance market rates for 2020 reflect stabilized markets, according to information released today by the Minnesota Department of Commerce in advance of the open enrollment period beginning November 1.
OK, my math here is gonna be a bit sloppy, but I'm just trying to illustrate a larger point about how splitting risk pools is, generally speaking, a Bad Thing.
Under the Affordable Care Act, non-ACA compliant healthcare policies were given until December 31st, 2013 to become fully ACA-compliant, including the new regulations mandating guaranteed issue, community rating, essential health benefits, no more annual or lifetime limits on coverage and so forth. All major medical policies offered from that day forward had to be fully ACA compliant (although there were some exceptions for short-term plans and so forth).
However, there was an exception made: Any existing policy which someone had been continuously enrolled in since before the ACA was signed into law by President Obama in March 2010 was considered to be "grandfathered" in. As long as the insurance carrier chose to keep offering those non-compliant policies, existing enrollees could remain enrolled, although premiums would of course increase from time to time. The "locked in" pool of enrollees would gradually dwindle as enrollees died, aged onto Medicare, got jobs with employer coverage and so on.
Former Wyoming Blackjewel LLC coal miners who have been out of work since July 1 and without health insurance since their group health plan was canceled Aug. 31 can sign up for the federal health insurance marketplace retroactively to Sept. 1.
The Wyoming Department of Insurance has successfully lobbied the Centers for Medicare and Medicaid Services (CMS) to make an “exceptional circumstances” special enrollment period through Oct. 30, said Denise Burke, an attorney with the state Department of Insurance.
The exception allows former Blackjewel coal miners an option to buy health insurance off the marketplace and made it retroactively effective to Sept. 1, which means workers and family members with ongoing health issues can continue treatment as if they never lost insurance.
LAS VEGAS (KLAS) — In a statement issued by Nevada Health Link, the organization announced that it had become aware that the Federal Health Insurance Marketplace, known as HealthCare.gov had incorrectly sent notices to Nevada consumers regarding the upcoming open enrollment period.
The incorrect notices were sent to Nevada consumers via mail, email and through notices on the HealthCare.gov portal.
"These notices from the Marketplace were sent in error. Nevadans who received these notices from the Marketplace should be aware that NevadaHealthLink.com is the only place to get enrolled in a qualified health plan during the next open enrollment period beginning on November 1, 2019," said Heather Korbulic, Executive Director for the Silver State Health Insurance Exchange.
Nevada consumers are asked to reach out to the Nevada Health Link consumer assistance center for further questions by calling 1-800-547-2927.
Back in June, I noted that the Michigan legislature was trying to slap a band-aid on the terrible GOP-passed & signed Medicaid work requirement bill (aka "God's Safety Net" bill) which passed about a year ago.
As you may recall, the original bill added fairly draconian work requirements to Michigan's implementation of the ACA's Medicaid expansion program, known here as "Healthy Michigan". Around 670,000 Michiganders are covered by the program (the number fluctuates between around 650K - 700K from week to week) today.
At the time, several reports had come out putting the number of people likely to lose healthcare coverage under the new requirements (which go into effect on January 1st, 2020) as high as 183,000 statewide, or as much as 28% of the total covered population...thousands of whom would lose coverage even if they do comply with the rules but aren't able to comply with the reporting requirements.
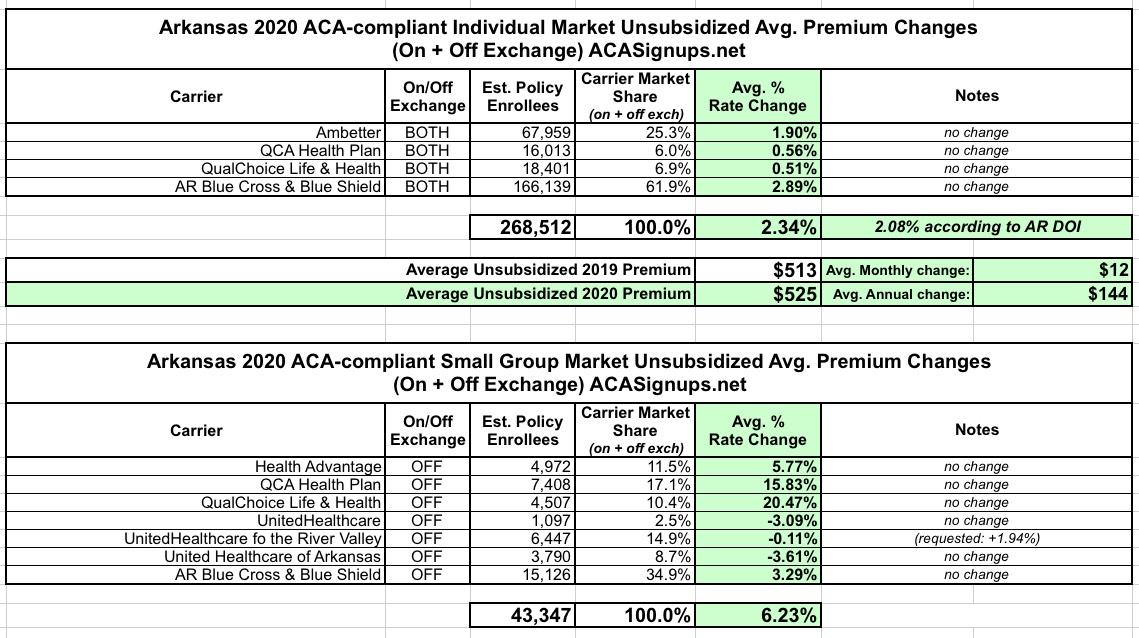
The Arkansas Insurance Dept. just posted their approved 2020 individual and small group market premium rate change requests. For the most part it's pretty straightforward: Individual market premiums are increasing about 2.3% statewide, while small group plans are going up 6.2% overall. This is virtually unchanged from their preliminary rate requests in July, although a single small group carrier had their request reduced from +2% to -0.1%, lowering the overall weighted average by a mere 0.2 points: