

ACA 2.0: Illinois (IL-14): How much would #HR1868 lower YOUR premiums?
Fri, 11/01/2019 - 1:12am
Back in March I wrote an analysis of H.R.1868, the House Democrats bill which comprises the core of the larger H.R.1884 "ACA 2.0" bill. H.R.1884 includes a suite of about a dozen provisions to protect, repair and strengthen the ACA, but the House Dems also broke the larger piece of legislation down into a dozen smaller bills as well.
Some of these "mini-ACA 2.0" bills only make minor improvements to the law, or in ways which are important but would take a few years to see obvious results. Others, however, make huge improvements and would be immediately obvious, and of those, the single most dramatic and important one is H.R.1868.
The official title is the "Health Care Affordability Act of 2019", but I just call both it and H.R.1884 (the "Protecting Pre-Existing Conditions and Making Health Care More Affordable Act of 2019") by the much simpler and more accurate moniker "ACA 2.0".
The official lead sponsor of H.R.1868 is Rep. Lauren Underwood (IL-14). While it currently only has 35 cosponsors, the larger H.R.1884 bill which includes H.R.1868 has 160 total sponsors to date, so there's no problems in terms of strong support within the Democratic caucus.
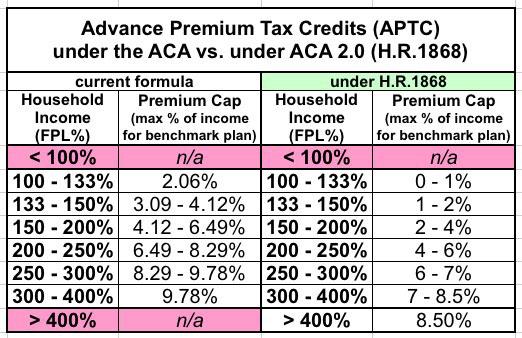
H.R.1868 itself is a very short and simple bill which does just two things, both of which involve changes to the current formula for ACA individual market subsidies:
- First, it removes the current tax credit maximum income eligibility threshold of 400% of the Federal Poverty Line (around $50,000/year if you're single, or $100,000/year for a family of four).
- Second, it makes the underlying formula for the tax credits more generous: Instead of the maximum amount the enrollee has to pay for a benchmark Silver plan ranging from around 2.1% of their income up to around 9.8%, H.R.1868 would drop this down to between 0% - 8.5% of income at the outside.
This may not sound like much, but it would make a huge difference for millions of Americans. The main beneficiaries would be the middle class...people earning too much to qualify for subsidies today, but not enough to easily afford ACA-compliant policies (basically, between 400 - 800% FPL). However, many of those who are already receiving subsidies would also see additional savings.
It's important to keep in mind that there are three main trouble spots when it comes to the individual market under the ACA: Premiums (mostly for the unsubsidized); deductibles/co-pays (for those earning more than 200% FPL); and provider network width. H.R.1868 addresses the first of these three, and it does so very well.
There are other provisions in the larger "omnibus" ACA 2.0 bill (and especially in the Senate version, S.1213) which deal with the other two, but for this project I'm only looking at the first: High premiums.
When I ran the numbers for my March analysis of H.R.1868, I used the national average premiums for Silver plans, which cover around 70% of the average person's medical expenses per year. However, that premium can vary greatly from state to state, county to county, carrier to carrier and even by the specific Silver plan you're looking at.
The actual measure is to look at the benchmark plan for the specific geographic area that the enrollee(s) live in. Under the ACA, the benchmark plan is the second lowest-cost Silver plan available on the ACA exchange.
It's important to understand that in addition to where they live, the benchmark plan premium will also vary greatly depending on...
- The number of people living in the household; obviously it will be different for a single adult vs. a family of four.
- The age of the enrollees: Unless you live in New York or Vermont, a millennial will cost a lot less than a baby boomer.
- In some states, children under 18 are eligible for CHIP or Medicaid at lower income levels even if the parents aren't.
- In states which have refused to expand Medicaid, those who earn 100-138% FPL are also eligible for extremely generous private plan subsidies.
- In Alaska and Hawaii, the FPL threshold is higher than in the rest of the country.
Therefore, I've decided to launch a new project: I'm going to run the numbers for H.R.1868 for all 435 Congressional Districts.
In terms of methodology, the first challenge is the geography. Most states have multiple premium rating areas (that is, carriers can charge different rates for the same plan in one vs. another within the state); not every carrier offers plans in every part of the state; and of course there's no connection between the insurance rating areas and Congressional District boundaries (especially with some gerrymandered districts winding their way from one end of the state to the other).
There's no perfect solution to this, but the best I've come up with is to use the highest-population zip code within each Congressional District (there's nearly 42,000 zip codes nationally).
Second: I have to account for the wide variance of household makeups. There's an endless array of possibilities, but I settled on eight specific households. Collectively, I think these are about as representative as I could reasonably be.
This is, needless to say, an extremely ambitious and time-consuming project, so I have no idea how long it will take. I might be able to post an entire state per day, or it might be only one or two districts at a time; we'll see how it goes.
I was planning on starting with my home state of Michigan, and already posted my analysis of the first two districts in the state...but then I realized that there's three other districts which I should start out with first: Rep. Lauren Underwood (IL-14), since she's the lead sponsor of H.R.1868; Rep. Frank Pallone (NJ-06), since he's the lead sponsor of the larger ACA 2.0 bill (H.R. 1884); and Richard Neal (MA-01), since he's the chair of the House Ways & Means Committee.
Illinois' 14th Congressional District, IL-14, covers the north & western suburbs of Chicago. Rep. Underwood lives in Naperville, Illinois, spanning both DuPage and Will Counties.
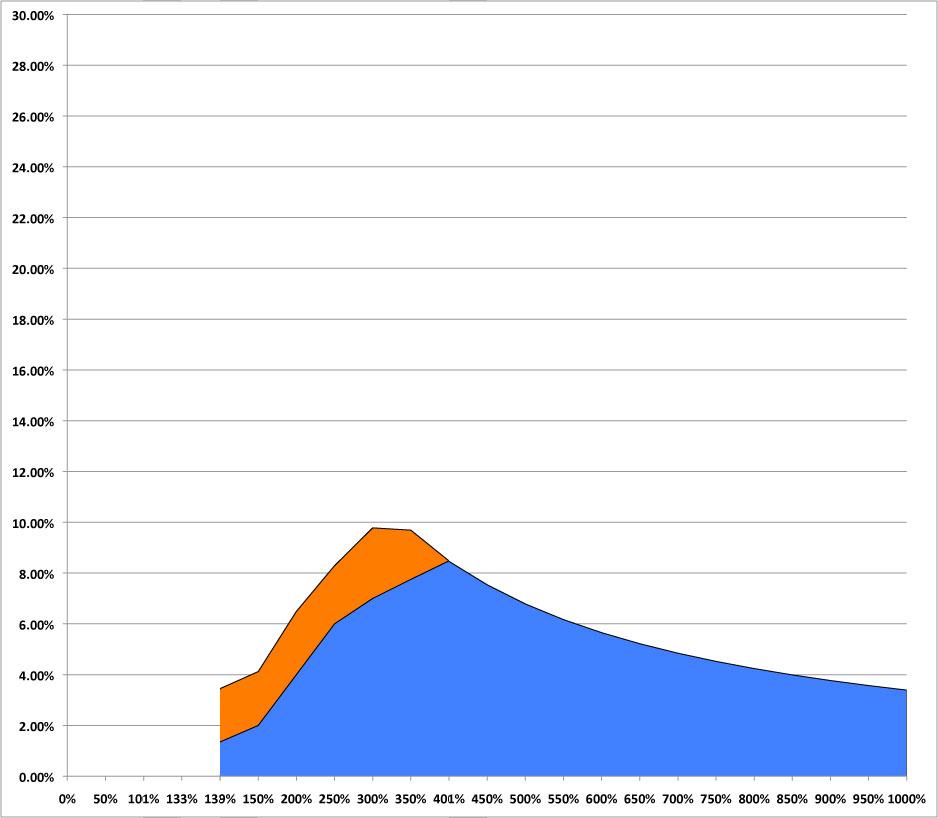
First up: A single 26-year old:
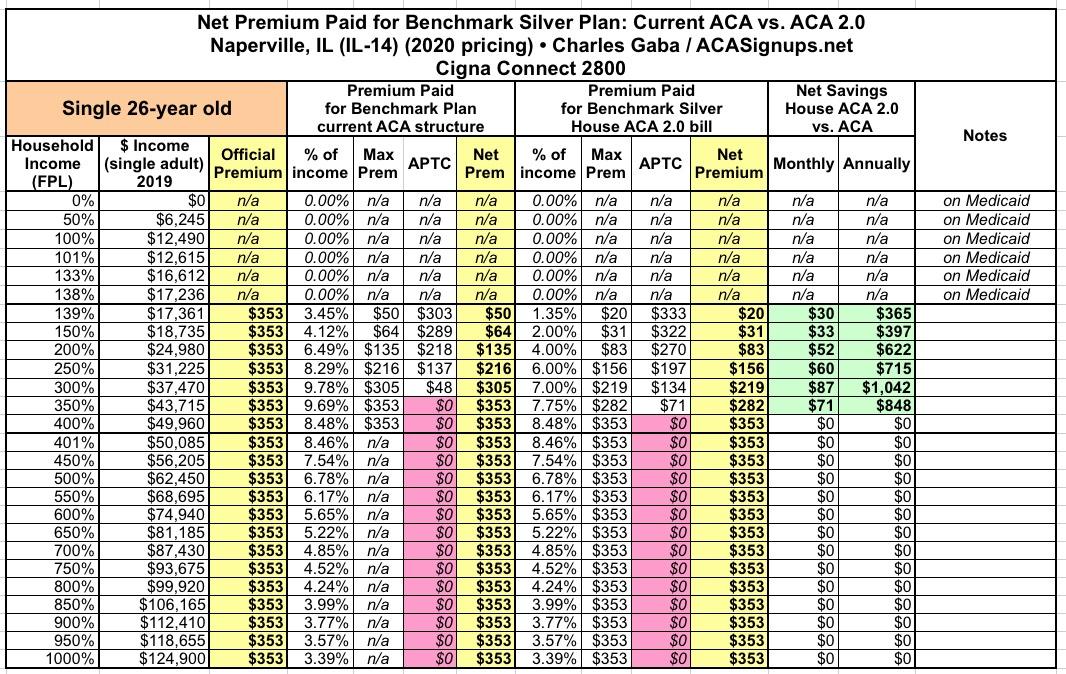
WIthout any subsidies, this young adult would be paying $353/month regardless of his or her income. Under the current ACA subsidy formula, they qualify for Medicaid up to an income of a little over $17,000/year. Over that their monthly premiums start at $50/month, then gradually increase to the full $353/month. In this case, that 400% FPL cap is never hit anyway, so removing it has no impact.
For those under 400% FPL, however, under H.R.1868, that $50/mo would drop down to $20/mo, and others in that range would save up to $87/month or $1,042/year.
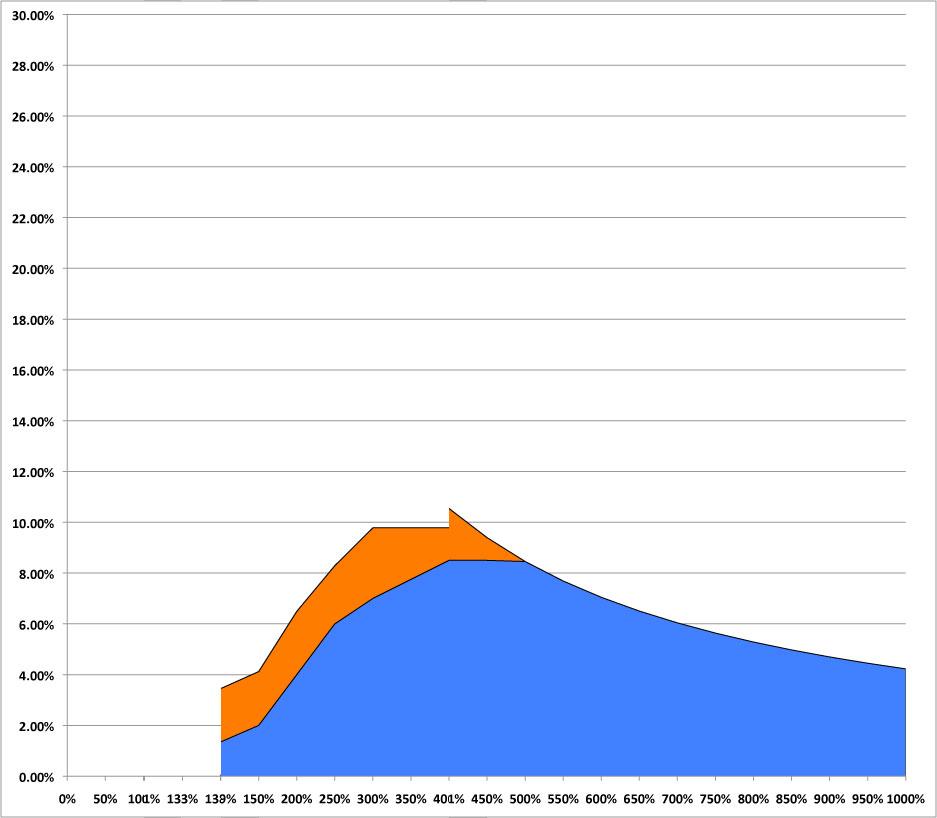
Next, the single 40-year old:
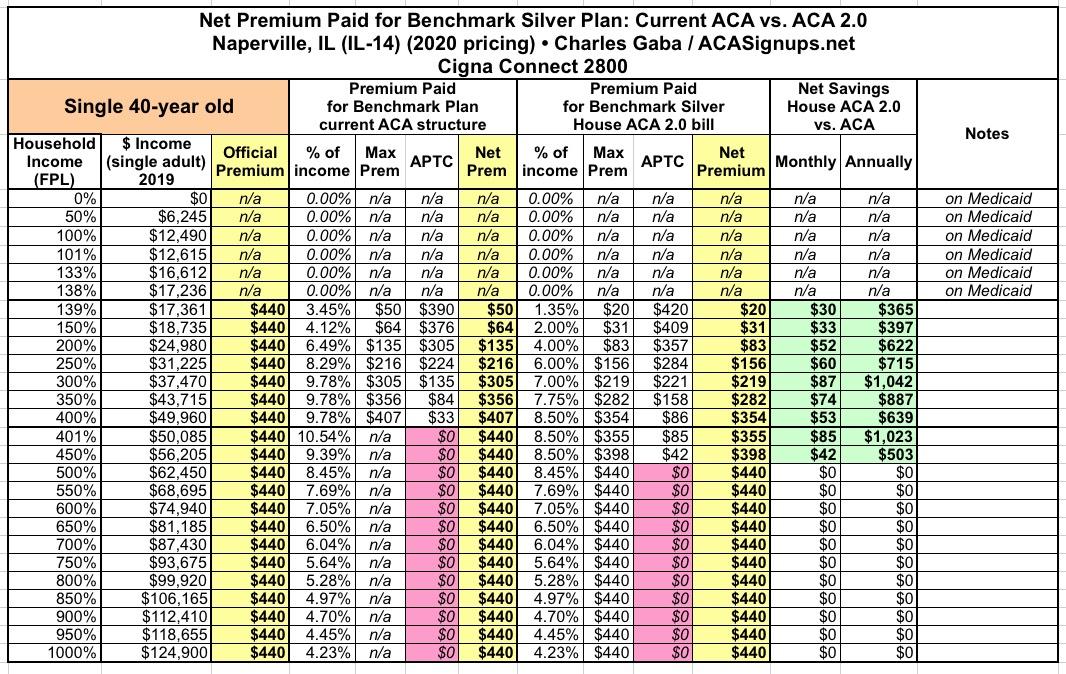
The savings for all of the single-person household would max out at just over $1,000/year regardless of their age...but as you can see, the older the enrollee, the more of a difference it makes as you move up the income scale. Thanks to the 8.5% cap (vs. 9.8%), those hovering around 400% and just over it can also save up to $1,000/year
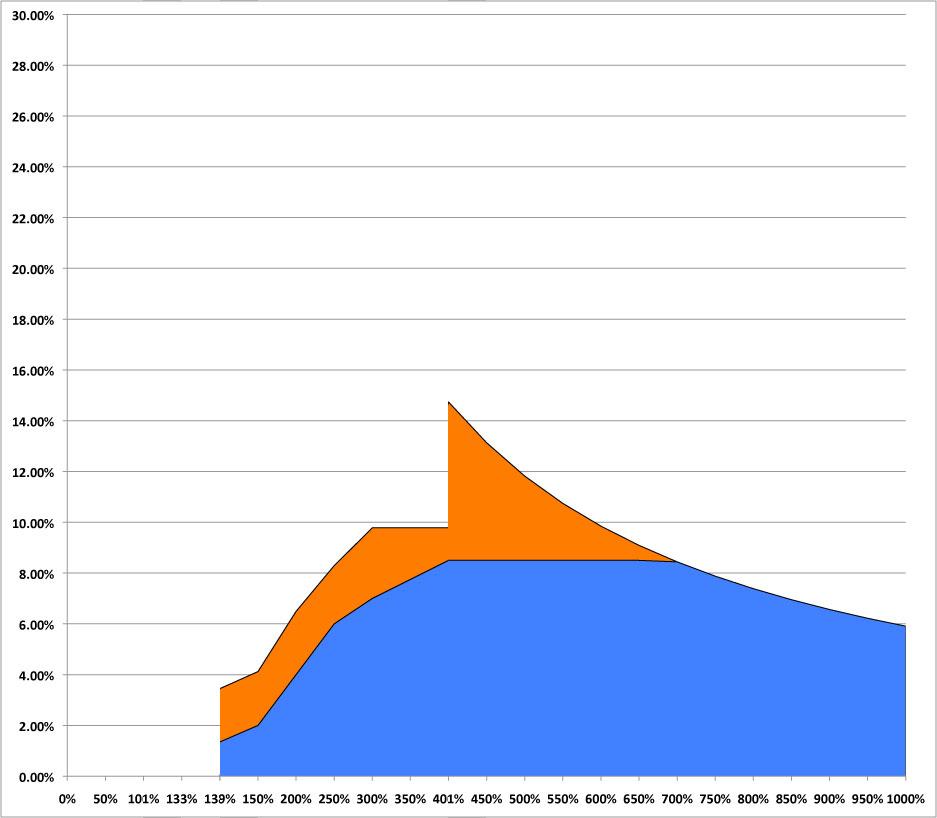
Next: A single 50-year old:
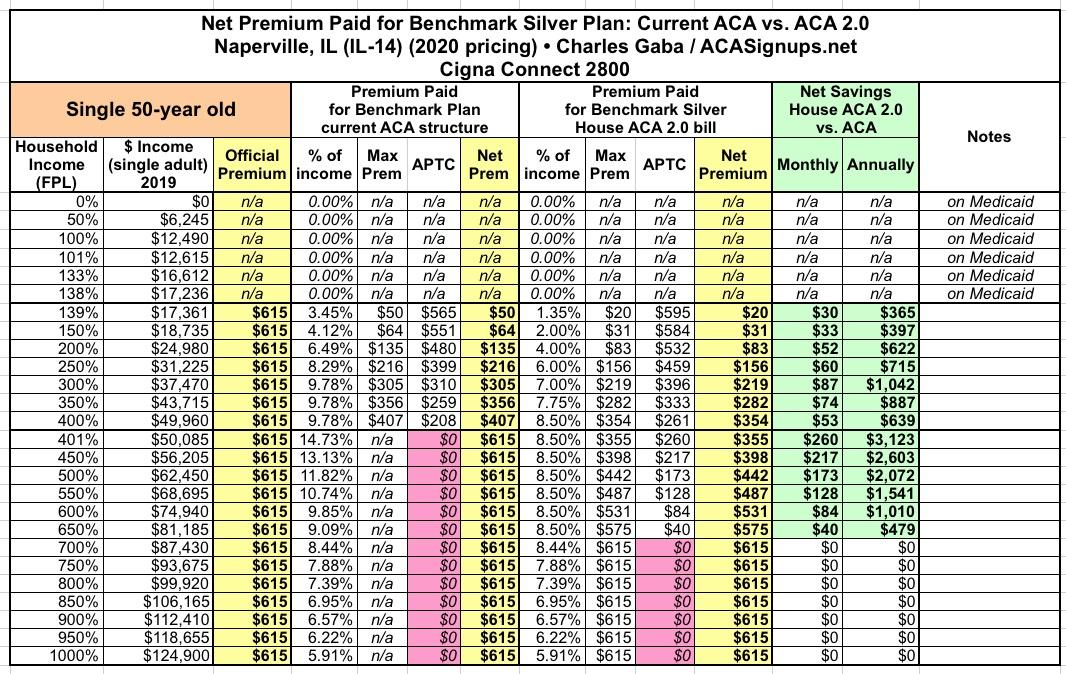
Here's where you can really see the infamous "subsidy cliff" start to kick in under the existing ACA formula. At exactly 400% FPL ($49,960/yr) they're eligible for $208/month in subsidies...but at 401%, they aren't eligible for anything. Under H.R.1868, they'd save as much as $260/month, saving up to $3,100/year as the more generous subsidies start to taper off naturally.
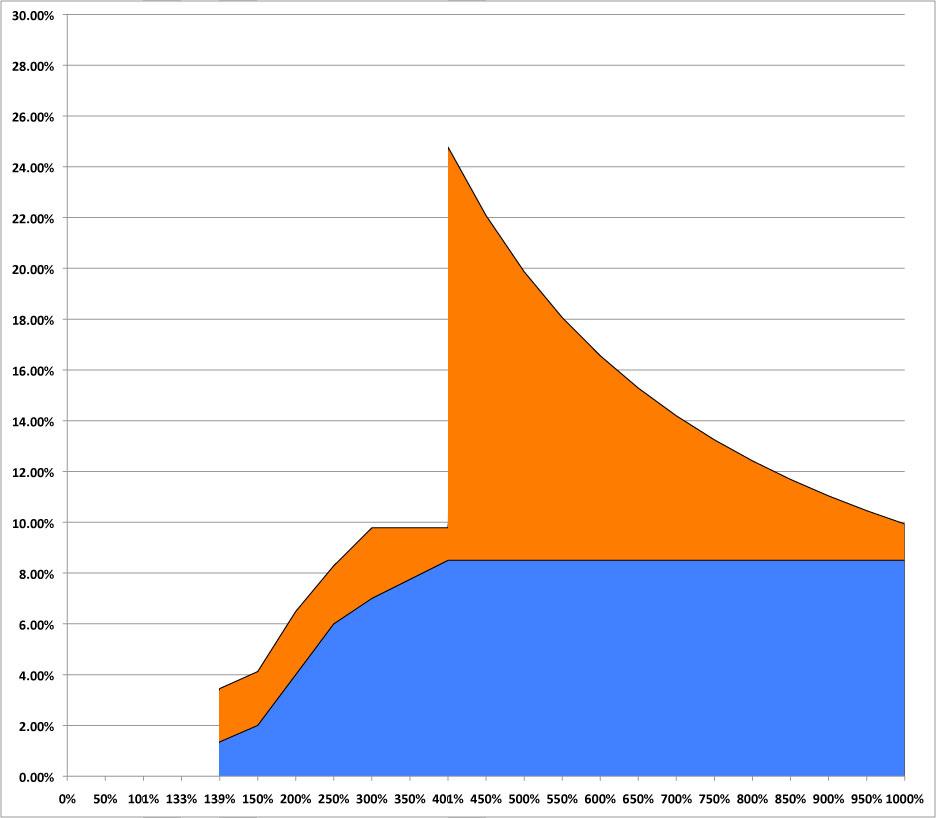
How about the pre-retirement 64-year old?
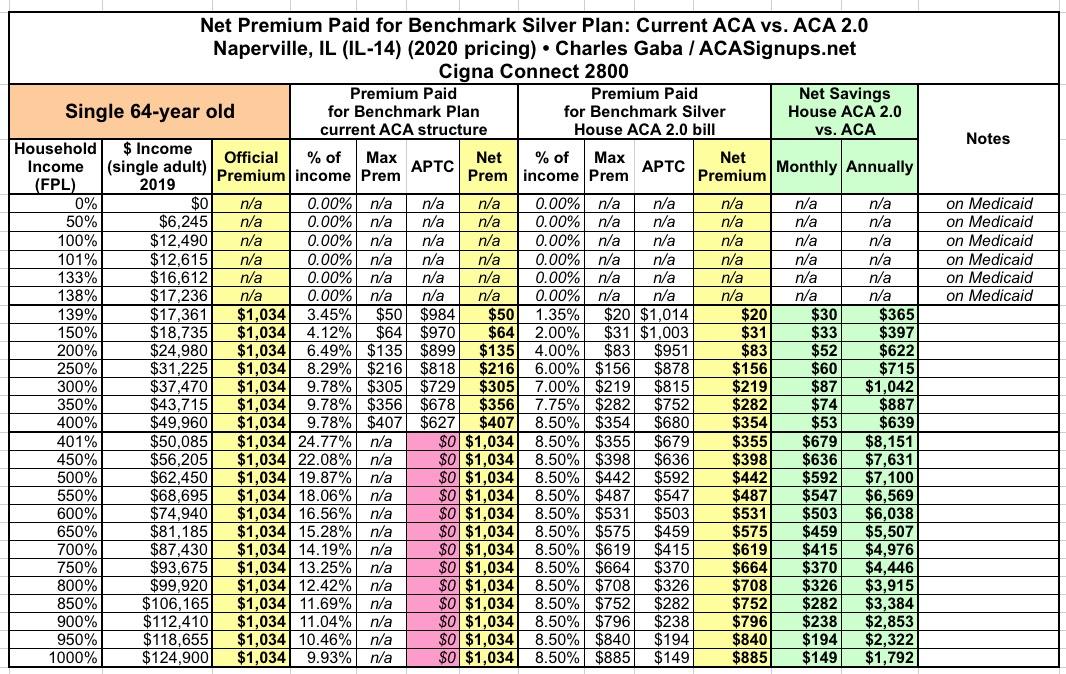
You can really see the Subsidy Cliff problem here. At 64 years old, they'd have to pay $1,034/month at full price...and with that 400% FPL cut-off, that'd eat up nearly 25% of their income.
Under H.R.1864, that would be cut down to just 8.5%, saving the enrollee up to $680/month or $8,100/year.
OK, so much for the single-person households. Let's move on to families.
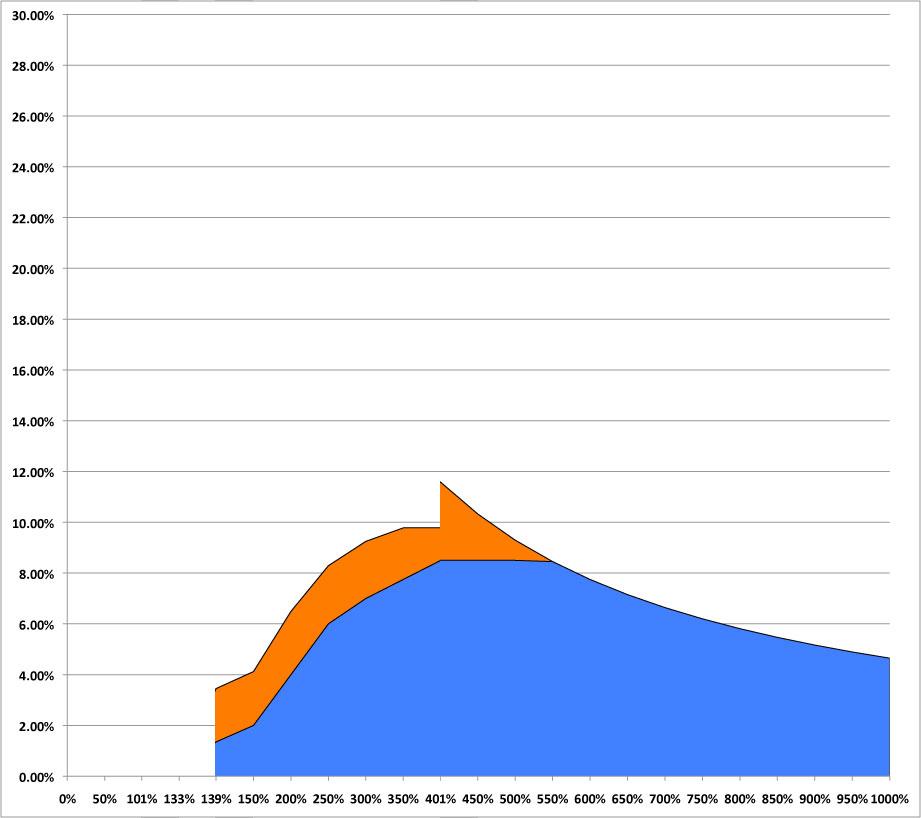
First, a 30-year old Single Parent with an 8-year old child:
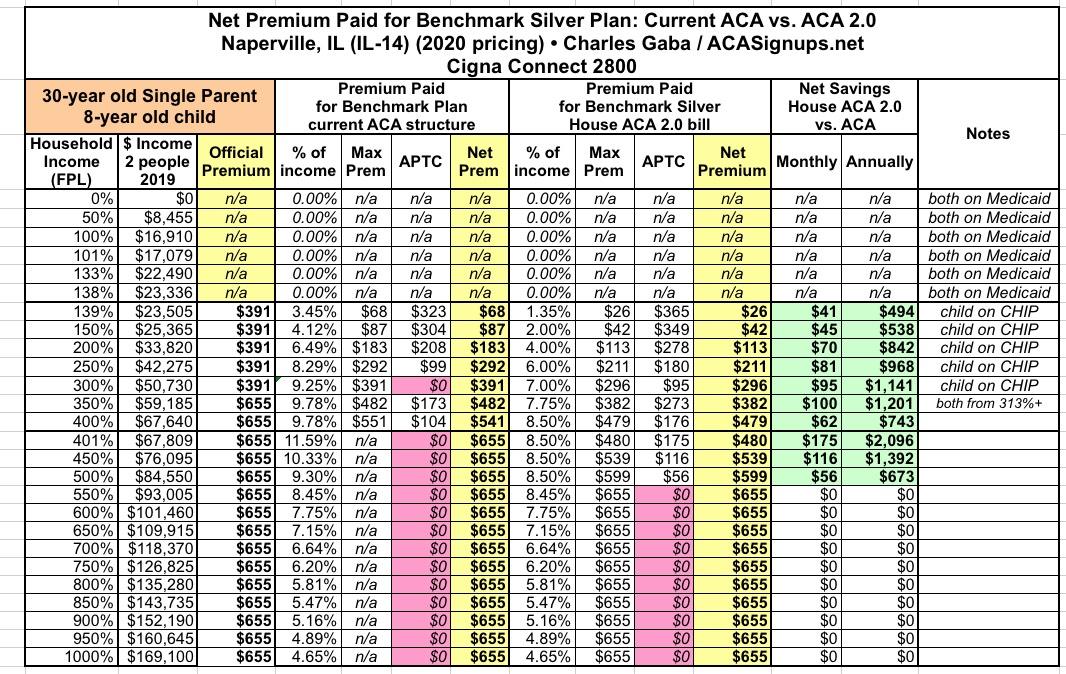
In Illinois, children qualify for CHIP up to 313% FPL, so the official premium for the parent only would only be $391 up through that point...but once their kid is added on, it jumps to $655/month. Under H.R.1868, they'd save up to $2,100/yr.
Next: The Nuclear Family: A 40-year old married couple with two children aged 12 & 10 (the age of the kids doesn't really matter until they hit 14, actually).
![]()
Again, the kids would be on CHIP until the family hits 313% FPL, so the unsubsidized premium for the parents only would run $881/mo. Over that, it's $1,408/month for all four of them.
Currently, once the family breaks the 400% threshold, premiums run as much as 16% of their income. Under H.R.1868, this would drop to 8.5%, saving them as much as $677/mo or over $8,100/year...and they'd still save up to $2,100/yr even if they already receive assistance.
![]()
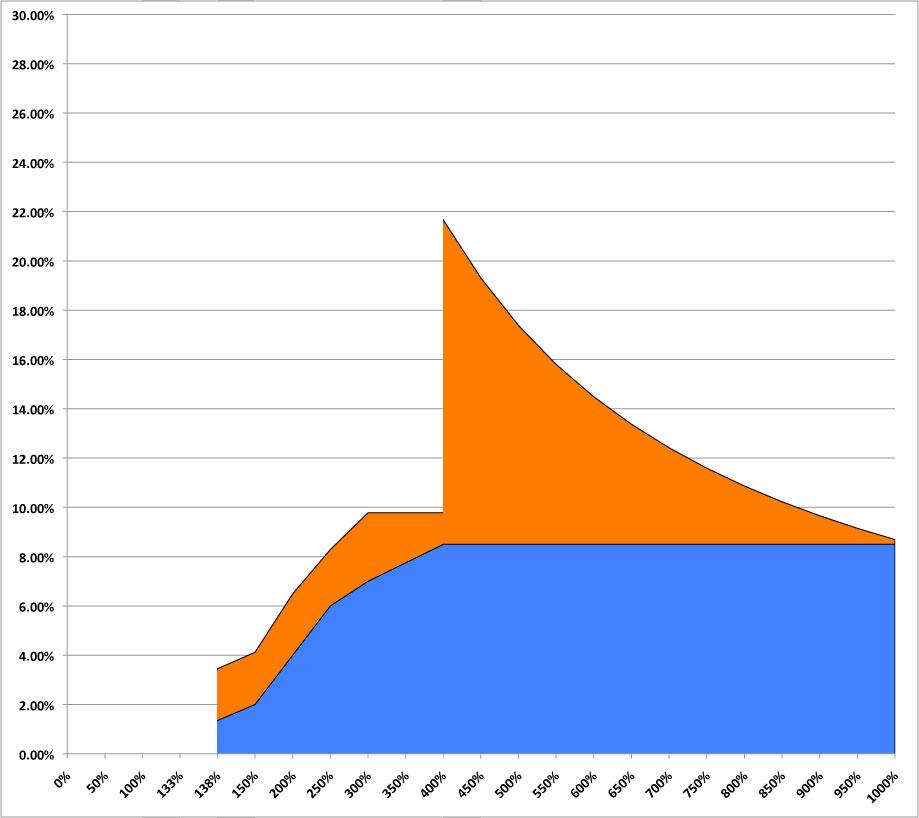
How about a 50-year old couple with a 18-year old kid still enrolled in their family plan (thanks to the ACA for that as well, I should note!)?
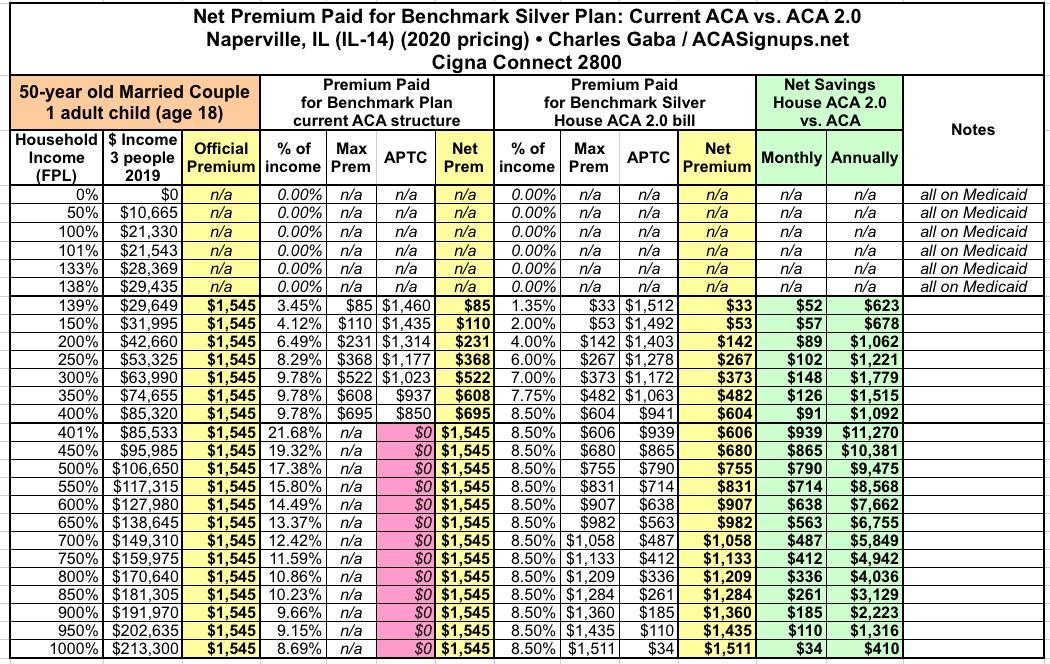
Currently, they'd have to pay up to 21% of their income over the cliff...under ACA 2.0, this is cut to 8.5%, saving them as much as $11,200/year, or up to nearly $1,800 if they're below the cliff level.
IMPORTANT: Note that the once their child turns 19, the rules regarding how subsidies are handled for adult children who aren't declared as dependents can get trickier.
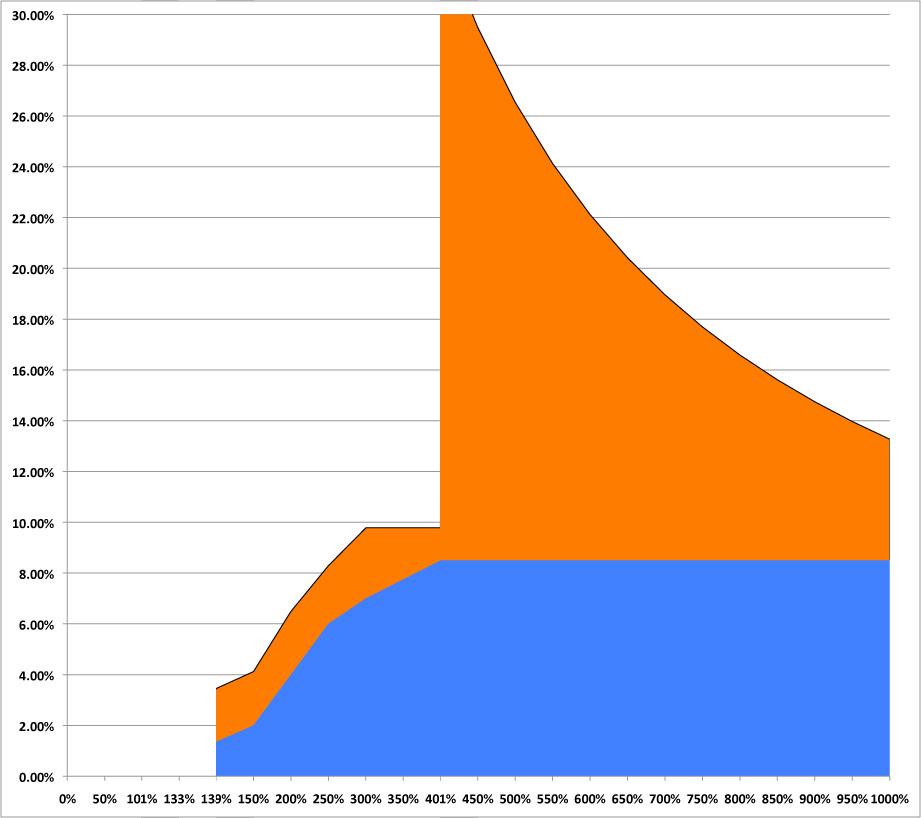
Finally, let's look at a 60-year old couple buying a policy for just the two of them:
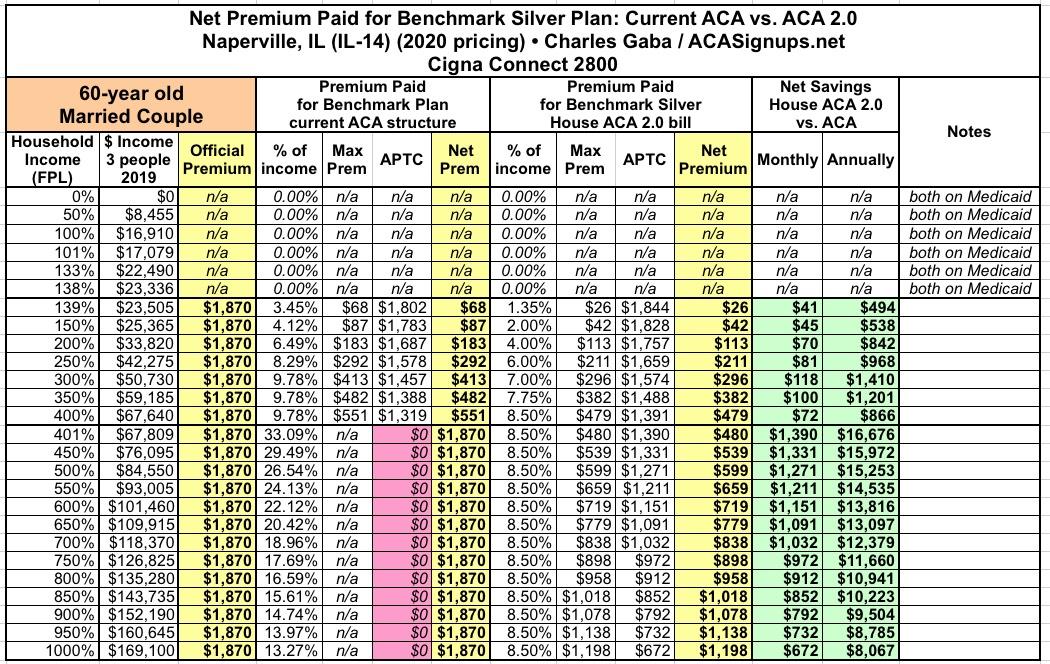
Under the current ACA formula, if they earn between $68,000 and, say, $140,000/year, this couple is almost certainly not going to buy any ACA plan unless one of them has extremely expensive conditions...at full price they'd have to pay as much as an absurd 33% of their income in premiums alone.
Under ACA 2.0, again, they'd pay no more than 8.5% in premiums, reducing their net premiums from $1,870/month down to as little as $480/month, a reduction of a whopping $16,600/year.
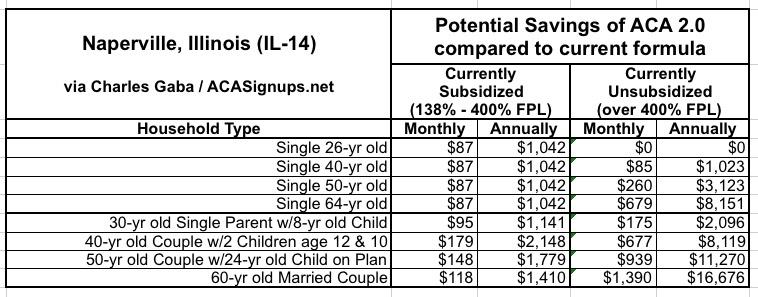
I've summarized all eight of the above tables into a single table below:
Advertisement
